science
Auditory cortex and phantom sound: why your brain rings when nothing does
Tinnitus is generated centrally even when triggered peripherally. fMRI and MEG studies of the auditory cortex point to maladaptive plasticity as the dominant model.
Published May 21, 2026 · By the EarLabs editorial desk
The peripheral trigger and the central generator
When someone develops tinnitus after a loud concert, it is tempting to locate the problem entirely in the ear. The cochlea was exposed to damaging sound levels; hair cells were injured; ringing started. The chain seems complete.
But the chain is not complete. Researchers using imaging technologies that can measure brain activity have found that people with chronic tinnitus show measurable differences in how their auditory cortex functions, differences that persist even when the ear is quiet, even in silence, and even in people who have had both auditory nerves severed in cases of severe tumor surgery. In some of those cases, tinnitus continues after the auditory nerve is cut.
This is one of the clearest lines of evidence that tinnitus is not just an ear problem. The brain, and specifically the auditory cortex, is a central player in generating or sustaining the phantom sound.
What the auditory cortex normally does
The auditory cortex occupies the superior temporal gyrus of each hemisphere. It receives signals from the auditory nerve via the brainstem and thalamus, and it performs the higher-level processing that converts raw frequency information into meaningful sound: pitch, timbre, spatial location, and, with help from other cortical regions, meaning.
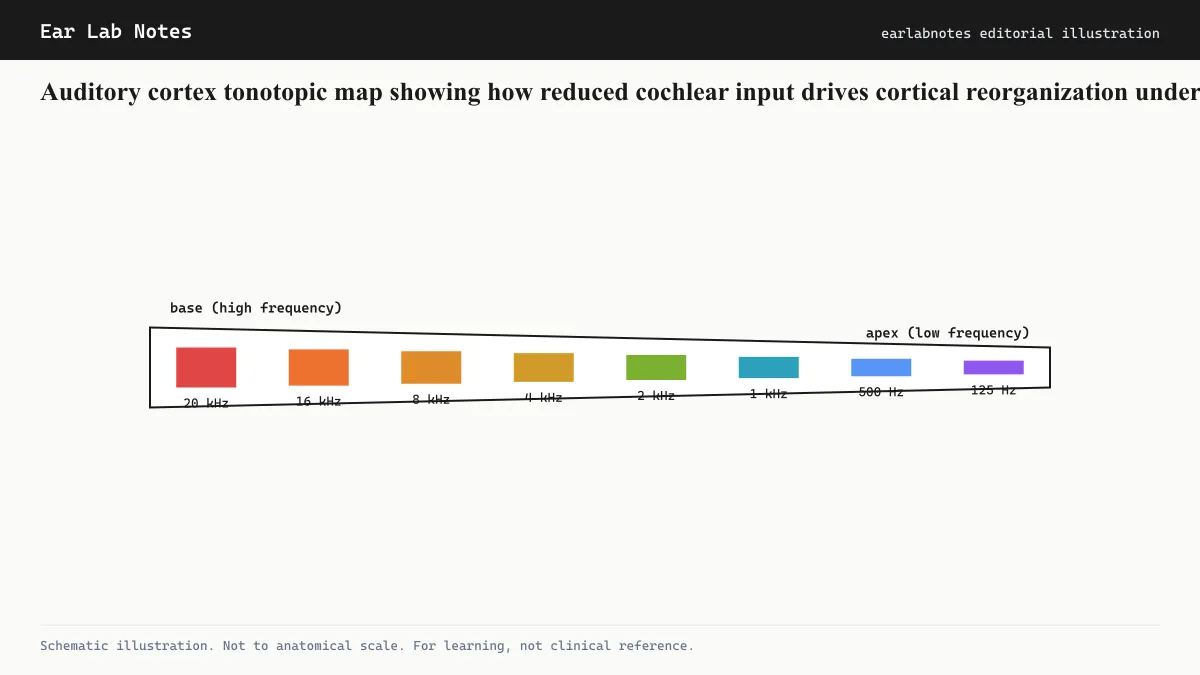
Like the cochlea, the auditory cortex is tonotopically organized. Neurons in one part of the cortex respond preferentially to high-frequency sounds; neurons in another area respond preferentially to low-frequency sounds. This cortical tonotopic map mirrors the cochlear tonotopic map and is maintained by the ongoing pattern of inputs arriving from the ear.
The cortical map is not fixed. It changes in response to experience, a property called cortical plasticity. Musicians who spend years processing particular instruments show expanded cortical representation of those instruments’ frequency ranges. The reverse also happens: when input from a frequency region is reduced or lost, the cortical map can reorganize.
What happens when cochlear input is lost
When cochlear hair cells in a particular frequency region are damaged or destroyed, the auditory nerve fibers serving that region stop conveying normal input to the cortex. The cortical neurons that used to receive those signals do not simply go silent. Research suggests several things happen instead.
First, cortical neurons that lost their normal input may become spontaneously active, firing without being driven by genuine sound. This spontaneous activity could be interpreted by the brain as a real signal at the corresponding frequency, producing phantom sound.
Second, neighboring cortical areas can invade the deafferented zone through a process called cortical map reorganization. Neurons previously tuned to adjacent frequencies begin to represent the damaged frequency region. This reorganization appears to involve both the sprouting of new connections and changes in inhibitory signaling.
This model, often called maladaptive plasticity, is not unique to hearing. Phantom limb pain, the perception of pain in an amputated limb, involves analogous reorganization in the somatosensory cortex. The auditory cortex appears to generate phantom sound through a parallel process.
NIDCD-supported research programs have invested substantially in understanding these cortical changes, because they represent potential targets for future interventions: if the abnormal cortical activity can be identified precisely and selectively modified, the tinnitus signal might be reduced.
Evidence from imaging studies
Functional MRI measures blood-oxygen-level-dependent (BOLD) signals as a proxy for neural activity. MEG measures the magnetic fields generated by neural currents directly, with higher temporal resolution.
Studies using both methods have found:
- Elevated spontaneous activity in auditory cortex regions corresponding to the tinnitus pitch.
- Abnormal synchrony between neurons at the tinnitus frequency.
- Changed patterns of connectivity between auditory cortex and non-auditory regions, including the limbic system.
- Cortical tonotopic shifts in people with noise-notch hearing loss and tinnitus, compared to those with hearing loss but without tinnitus.
The last finding is particularly relevant. Having the same audiometric hearing loss pattern is not sufficient to predict tinnitus. The cortical response to that hearing loss appears to matter, which raises the question of why some brains reorganize in ways that produce tinnitus and others do not.
Central gain: the volume knob hypothesis
A related model describes the process in terms of central gain. When peripheral input is reduced, the central auditory pathway compensates by amplifying its response to whatever input it does receive. This is analogous to turning up a radio’s volume when the signal is weak. The amplification is useful in principle: it prevents the cortex from simply going dark when input is lost.
The problem is that amplifying internal noise, the spontaneous electrical activity that is always present in neural tissue at low levels, produces an output that resembles a real sound. The central-gain hypothesis proposes that tinnitus is this amplified internal noise, a consequence of the auditory system’s attempt to compensate for lost input.
This model has practical implications. If tinnitus is partly a gain problem, then restoring real auditory input (through hearing aids or cochlear implants in appropriate candidates) should reduce the drive to amplify. Several lines of clinical evidence suggest this happens, at least partially.
The non-auditory involvement
The auditory cortex does not operate in isolation. Tinnitus distress, the degree to which tinnitus is bothersome rather than merely present, correlates with activity in limbic structures including the amygdala and hippocampus. People who are highly distressed by their tinnitus show more cross-talk between auditory and limbic networks than people with similar audiometric profiles who are not distressed.
This is why AAO-HNS clinical guidelines recommend psychological intervention (particularly CBT) as part of tinnitus management even though CBT does not target the auditory cortex directly. By reducing the limbic system’s reactivity to the tinnitus signal, CBT appears to reduce the salience of the phantom sound without changing the cortical activity that generates it.
What this means for treatment research
Understanding that tinnitus is centrally generated has redirected a significant portion of tinnitus research toward central targets. These include:
- Neuromodulation approaches (TMS, tDCS, vagus nerve stimulation) aimed at disrupting the cortical oscillations associated with tinnitus
- Pharmacological targets aimed at restoring inhibitory signaling in the auditory cortex
- Hearing-device approaches that aim to provide rich auditory input and normalize central gain
None of these has yet produced a broadly effective treatment for chronic subjective tinnitus. As of current clinical guidelines, the evidence-based management options remain behavioral and sound-based rather than neurophysiologically targeted. But the understanding of the cortical mechanisms has advanced substantially and continues to drive research programs at institutions including NIDCD.
If symptoms persist or change, see an audiologist or physician.
Frequently asked questions
- Is tinnitus a brain problem or an ear problem?
- Most researchers currently view tinnitus as a central auditory phenomenon that is often triggered by peripheral (cochlear) events. The ear may provide the initial damage, but the sustained ringing appears to be generated or amplified in the brain's auditory processing areas.
- What brain imaging shows about tinnitus?
- fMRI and magnetoencephalography (MEG) studies have found altered activity patterns in the auditory cortex of people with chronic tinnitus compared to those without. These include changes in spontaneous firing rates, cortical tonotopic reorganization, and abnormal cross-frequency coupling. No single imaging finding is yet diagnostic for tinnitus.
- Can the auditory cortex change back after tinnitus develops?
- Cortical plasticity works in both directions. The brain changes in response to its inputs, and restoring normal auditory input through hearing aids or cochlear implants has been associated with reductions in tinnitus in some people. However, full reversal of cortical reorganization in established chronic tinnitus has not been demonstrated.
- Why do some people with identical hearing loss not have tinnitus?
- This is one of the key unsolved questions in tinnitus research. Peripheral hearing loss increases tinnitus risk but does not guarantee it. Researchers are investigating whether differences in central auditory gain regulation, limbic reactivity, and neural resilience explain individual variation.
- Does brain stimulation work for tinnitus?
- Transcranial magnetic stimulation and transcranial direct current stimulation have been studied as tinnitus treatments. Results from controlled trials are inconsistent, and neither is currently endorsed as a standard treatment by major clinical guidelines such as those from AAO-HNS.
EarLabs Notes
One short note a week. Tinnitus and hearing health.
New tools, plain-language summaries of recent research, no spam. Unsubscribe in one click.
No tracking pixels, no behavioral retargeting. Read our privacy notes.
Primary sources
- Tinnitus: Overview and Management — NIH/NIDCD
- Clinical Practice Guideline: Tinnitus — AAO-HNS
- Tinnitus: Symptoms and Causes — Mayo Clinic
- Tinnitus — NHS UK