causes
Blood pressure and tinnitus: pulsatile ringing, vascular noise, and what to ask your doctor
How high blood pressure, atherosclerosis, and vascular abnormalities can produce pulsatile tinnitus you can hear in time with your heartbeat.
Published May 21, 2026 · By the EarLabs editorial desk
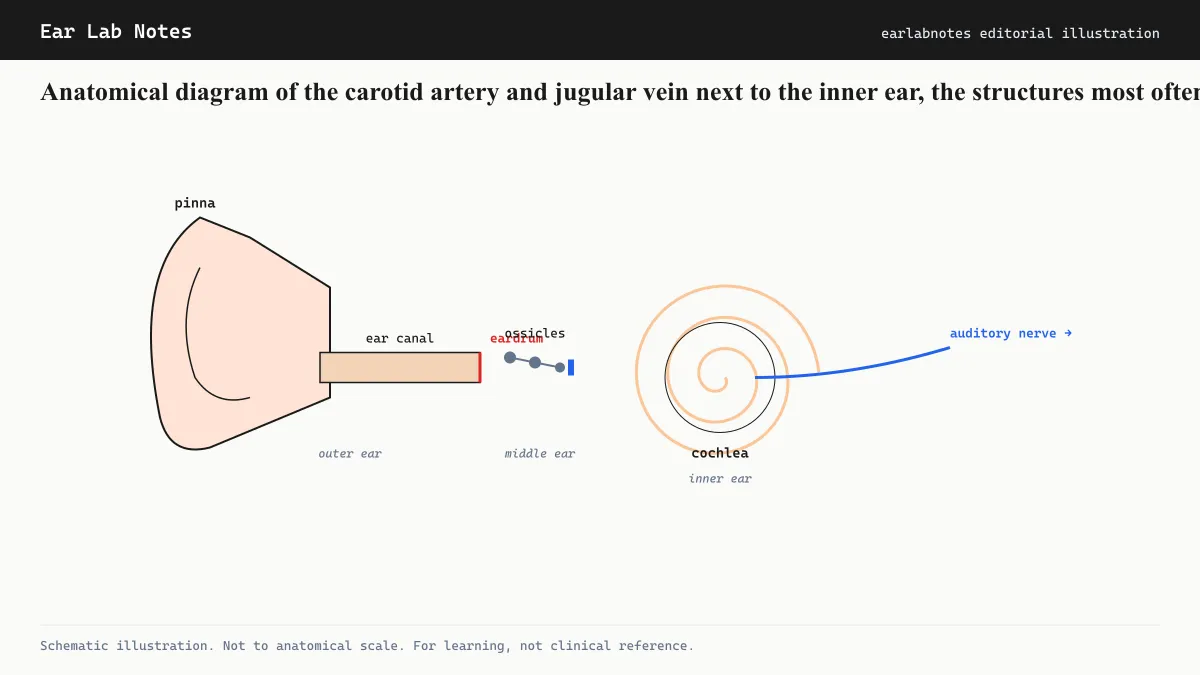
Most tinnitus is a phantom sound, generated by the auditory nervous system rather than by any actual physical sound source inside the body. Vascular tinnitus is different. It arises from real turbulent blood flow that is transmitted through bone and tissue to the inner ear, where it is perceived as sound synchronized with the heartbeat.
The relationship between blood pressure, vascular anatomy, and tinnitus is clinically important because it is one of the few forms of tinnitus that may be directly treatable by addressing its underlying cause.
What makes blood flow audible
Under normal conditions, blood moves through arteries and veins in a smooth, laminar flow that generates minimal turbulence and no perceptible sound. Several conditions disrupt this smooth flow and create turbulence that generates sound energy:
Elevated blood pressure: High blood pressure increases the velocity and force of blood passing through vessels near the inner ear. This can make the flow turbulent enough to transmit an audible pulse through the temporal bone to the cochlea.
Atherosclerotic narrowing: Plaques in the carotid artery or other vessels near the ear create a narrowed channel (stenosis) that significantly increases local flow velocity, producing turbulence even when resting blood pressure is controlled. The sound of turbulence through a narrowed carotid is called a carotid bruit.
Aberrant vessel anatomy: Some people have anatomical variants where vascular structures sit unusually close to the cochlea or middle ear. A high-riding or dehiscent jugular bulb (where the top of the jugular vein protrudes into or through the floor of the middle ear) is one recognized cause. An aberrant internal carotid artery that takes an unusual course through the middle ear is another.
Arteriovenous malformations and fistulae: Abnormal direct connections between arteries and veins bypass the normal capillary bed, creating high-flow turbulent channels. Dural arteriovenous fistulae near the ear are a recognized cause of pulsatile tinnitus that often requires specialist intervention.
Idiopathic intracranial hypertension
A distinct vascular mechanism involves elevated pressure in the cerebrospinal fluid (CSF) that surrounds the brain. Idiopathic intracranial hypertension (IIH), also called pseudotumor cerebri, raises the pressure in the fluid space surrounding the brain and the auditory structures. This elevated pressure is transmitted to the jugular veins and can produce a characteristic venous pulsatile tinnitus, often louder when lying down. IIH is more common in women of reproductive age who are overweight and can also cause headache and visual symptoms.
How pulsatile tinnitus differs perceptually
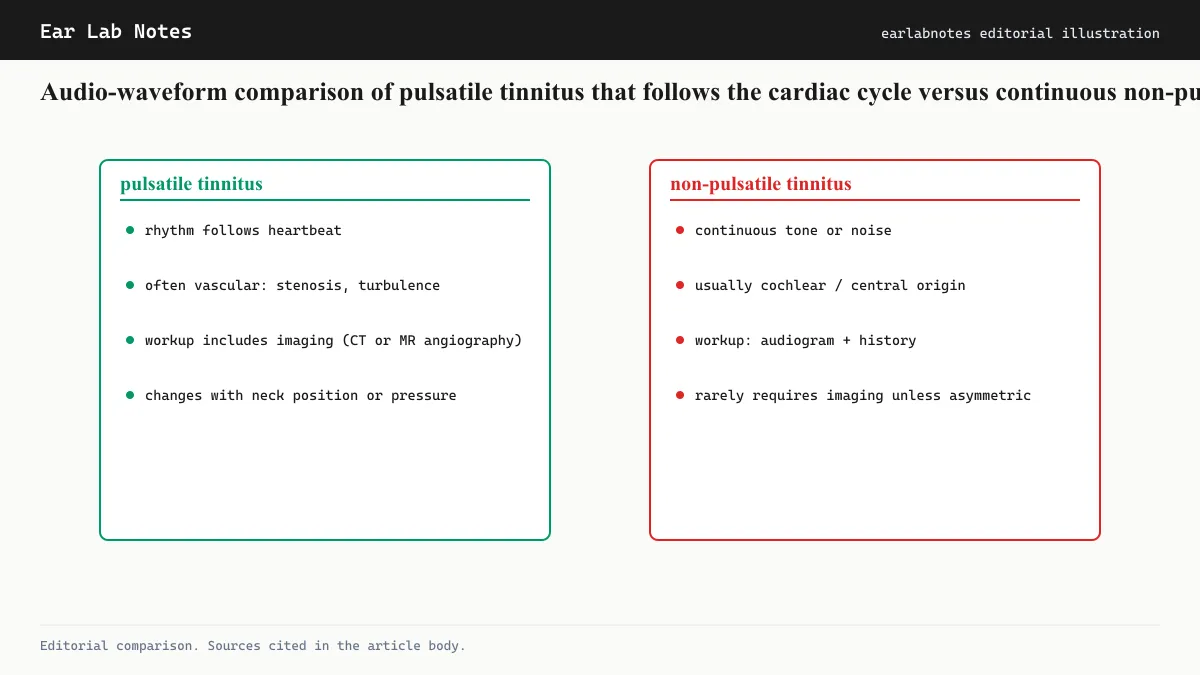
Pulsatile tinnitus follows the heartbeat. People with this form describe the sound as a rhythmic whooshing, thumping, or rushing that corresponds to their pulse. Some notice it most acutely when lying quietly, as external ambient noise is reduced and the internal sound becomes comparatively louder. Many can temporarily suppress it by pressing on the jugular vein on the affected side or by turning their head, which alters vascular flow.
Non-pulsatile (continuous) tinnitus, by contrast, persists without any cardiac synchrony and does not change with brief vascular maneuvers in this way.
Evaluation
Because pulsatile tinnitus has a range of causes from benign to requiring treatment, the clinical evaluation differs from that of ordinary tinnitus. AAO-HNS guidelines consider pulsatile tinnitus a condition warranting imaging in most cases. Standard evaluation may include:
- Blood pressure measurement (basic but essential)
- Auscultation of the neck and periauricular area for bruits
- Audiogram to assess whether cochlear hearing loss coexists
- CT or MRI angiography of the head and neck to assess vascular anatomy
- Assessment of CSF pressure if IIH is suspected
The goal of imaging is to identify or exclude vascular abnormalities that are treatable (stenosis, fistula, aberrant vessel) versus benign variants or hypertension-driven flow noise.
Blood pressure and tinnitus beyond the pulsatile form
Hypertension is also listed among the associated conditions in NIDCD’s tinnitus overview beyond pulsatile mechanisms. The basis for this broader association is less mechanistically clear. Some clinicians observe that uncontrolled hypertension appears to worsen subjective tinnitus, possibly through effects on cochlear blood supply, though this relationship is less precisely characterized than the pulsatile mechanism.
What to discuss with a clinician
If tinnitus beats in time with the pulse, or if it is new and accompanied by headaches, visual symptoms, or neck sounds, bringing these features to a clinician’s attention at the first visit is important. Describing the rhythm and any maneuvers that temporarily reduce or increase the sound helps the clinician prioritize the evaluation efficiently.
Tinnitus that does not have a pulsatile quality is far less likely to be vascular in origin, and the evaluation and management differ accordingly.
Anemia, thyroid disease, and other systemic causes of increased flow
Several general medical conditions increase cardiac output and blood-flow velocity without necessarily causing hypertension in the conventional sense, and these can produce pulsatile tinnitus through the same turbulence mechanism:
Anemia: Reduced red blood cell count forces the heart to pump faster and harder to deliver adequate oxygen. This increased output raises flow velocity in all vessels, including those near the ear. Pulsatile tinnitus from anemia typically resolves as the anemia is treated.
Hyperthyroidism: Excess thyroid hormone increases heart rate and cardiac output. High-output states from any cause can make venous flow near the ear turbulent enough to be heard.
Pregnancy: The physiological increase in blood volume and cardiac output during pregnancy is associated with pulsatile tinnitus in some cases. This is typically benign and resolves postpartum, but any new tinnitus during pregnancy warrants clinical evaluation to exclude IIH and other conditions.
What to tell your clinician
When reporting pulsatile tinnitus to a clinician, the following details are particularly useful: which ear or ears are affected, whether the rhythm follows the heartbeat, whether it changes with body position (louder when lying down is consistent with venous or IIH causes), whether pressing on the neck briefly reduces or stops the sound, and whether other symptoms (headache, visual changes, neck pain) accompany it. This information helps direct the evaluation efficiently.
If symptoms persist or change, see an audiologist or physician.
Frequently asked questions
- If I control my blood pressure, will my pulsatile tinnitus go away?
- In cases where hypertension is the primary driver of pulsatile tinnitus, blood pressure control can reduce or resolve it. However, pulsatile tinnitus has many potential causes, some of which are not blood-pressure-related. A clinician should evaluate the tinnitus before assuming hypertension is the sole cause, because some vascular causes require specific treatment independent of blood pressure management.
- Should pulsatile tinnitus always be investigated?
- Yes. AAO-HNS guidelines and Mayo Clinic both recommend imaging evaluation for pulsatile tinnitus to identify vascular or structural causes that may need treatment. While many cases turn out to be benign, a small subset involve conditions such as arteriovenous malformations or dural arteriovenous fistulae that benefit from targeted intervention.
- Can pulsatile tinnitus be heard by a doctor?
- In some cases, yes. A clinician listening with a stethoscope placed near the ear or neck may detect a bruit (an audible vascular turbulence) that corresponds to what the patient hears. This is one of the defining features of objective pulsatile tinnitus. Not all pulsatile tinnitus is audible externally, however.
EarLabs Notes
One short note a week. Tinnitus and hearing health.
New tools, plain-language summaries of recent research, no spam. Unsubscribe in one click.
No tracking pixels, no behavioral retargeting. Read our privacy notes.
Primary sources
- Tinnitus - NIDCD — National Institute on Deafness and Other Communication Disorders
- Tinnitus - Mayo Clinic — Mayo Clinic
- Clinical Practice Guideline: Tinnitus - AAO-HNS — American Academy of Otolaryngology, Head and Neck Surgery
- High Blood Pressure - NHS — NHS UK