management
Cochlear implants and tinnitus: when restoring input quiets phantom sound
Most cochlear implant recipients report reduced tinnitus in the implanted ear. The leading explanation is that restored auditory input downregulates central gain. Evidence and exceptions.
Published May 21, 2026 · By the EarLabs editorial desk
Cochlear implants are not tinnitus treatments. They are devices approved for severe to profound sensorineural hearing loss when hearing aids no longer provide adequate benefit. But a consistent pattern in the clinical literature has caught the attention of researchers: a large proportion of cochlear implant recipients report that their tinnitus is reduced in the implanted ear after activation.
Understanding why this happens, how reliably it happens, and what it means for people with both hearing loss and tinnitus is useful background knowledge.
How a cochlear implant works
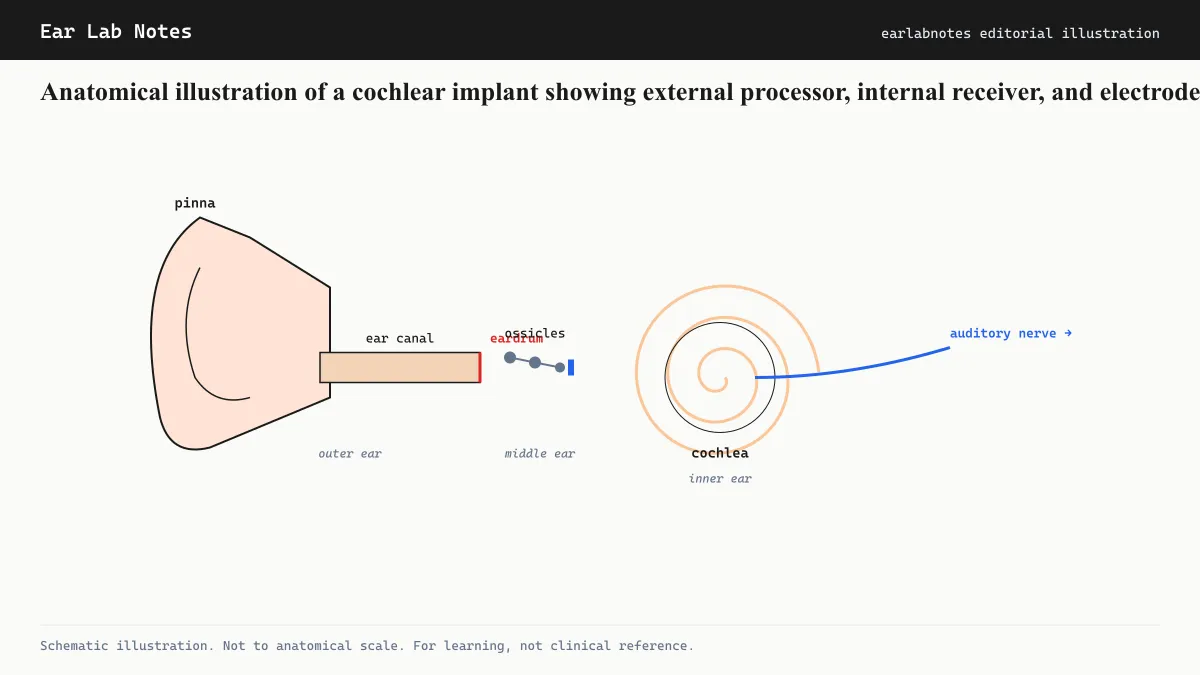
A cochlear implant bypasses the damaged hair cells of the cochlea entirely. The device consists of an external sound processor that sits behind the ear, a transmitter coil held against the scalp by a magnet, and an internal receiver-stimulator implanted in the bone behind the ear. The internal component connects to an electrode array threaded into the cochlea.
When the external processor captures sound, it converts it into digital signals and transmits them through the skin to the internal receiver. The receiver converts these into electrical pulses delivered by the electrode array, which directly stimulates the auditory nerve fibers. The brain learns to interpret these electrical signals as sound.
The cochlear implant thus restores auditory input to the auditory nerve, and through it to the central auditory nervous system, even in cases where the hair cells are largely or entirely non-functional.
Why tinnitus often decreases after implantation
The central-gain hypothesis provides the most widely cited explanation for tinnitus reduction after cochlear implantation.
When the cochlea delivers less signal to the auditory nerve, the brain’s central auditory pathway compensates by increasing its sensitivity. This compensatory increase in neural gain, amplifying whatever signal exists, is thought to be the mechanism behind tinnitus: the auditory cortex amplifies its own internal noise into a perceptible phantom sound.
When a cochlear implant delivers structured electrical stimulation to the auditory nerve, it effectively restores meaningful input to the previously deprived pathway. The hypothesis is that this restoration of input allows the central auditory system to reduce its compensatory gain, which in turn reduces the amplification of internal noise that was generating the tinnitus.
This mechanism is consistent with what is observed behaviorally. Most implant recipients who report tinnitus reduction do so after the implant is activated and during periods of use. When the implant is switched off, tinnitus sometimes returns.
What the evidence shows
Several reviews and case series in the cochlear implant literature have described tinnitus outcomes. Across multiple studies, the majority of implant recipients who had pre-operative tinnitus report improvement or complete resolution of tinnitus in the implanted ear. Published figures vary across studies, but improvement rates above 50 percent and often above 70 percent are commonly reported.
Complete resolution (tinnitus disappearing entirely) is less common than partial improvement. Some recipients report that tinnitus is reduced but not eliminated, or that it fluctuates. A smaller proportion report no change or worsening, which is a finding clinicians discuss with candidates before surgery.
NIDCD acknowledges that cochlear implants can sometimes reduce tinnitus as a secondary effect of auditory restoration, though this is not listed as a primary indication.
Single-sided deafness and tinnitus
Single-sided deafness (SSD), where one ear has severe to profound loss and the other is normal or near-normal, is a specific population where cochlear implantation has attracted increasing attention partly because of tinnitus outcomes.
In SSD, tinnitus in the profoundly deaf ear often accompanies the hearing loss. Because hearing aids cannot meaningfully amplify sound in a profoundly deaf ear, they provide limited relief for the tinnitus side. Cochlear implantation in the deaf ear restores input and has been associated with meaningful tinnitus improvement in this population across several published series.
This finding has influenced candidacy considerations in some countries. The NHS and AAO-HNS have both seen evolving guidance around SSD and cochlear implantation, though criteria and coverage vary.
What cochlear implantation cannot do for tinnitus
A cochlear implant is a major surgical intervention requiring general anesthesia, a period of recovery, and an intensive rehabilitation program to learn to use the device. The indication is hearing loss, not tinnitus.
Nobody should consider cochlear implantation as a tinnitus treatment absent the audiometric criteria for implantation based on hearing loss. The evidence for tinnitus reduction is secondary. For someone with mild or moderate hearing loss and significant tinnitus, hearing aids with sound therapy programs are a more proportionate starting point.
The non-implanted ear’s tinnitus is generally not affected by unilateral implantation. Bilateral tinnitus in someone with bilateral severe hearing loss requires discussion of bilateral implantation, which is a different set of candidacy considerations.
Cochlear implants as part of a broader tinnitus conversation
For people who meet the audiometric criteria for cochlear implantation based on their hearing loss, the likelihood of tinnitus reduction in the implanted ear is a relevant secondary consideration worth discussing with the surgical team. It is not a reason to pursue implantation; it is useful context for understanding the full range of expected outcomes.
For people who are weighing cochlear implantation primarily because of tinnitus, the conversation needs to be redirected toward whether the hearing loss itself meets candidacy criteria.
If symptoms persist or change, see an audiologist or physician.
Frequently asked questions
- Do cochlear implants cure tinnitus?
- No. Cochlear implants are not indicated for tinnitus and are not approved as a tinnitus treatment. The reduction in tinnitus that many implant recipients report is a secondary effect of restoring auditory input, not the primary goal of implantation.
- Who qualifies for a cochlear implant?
- Cochlear implant candidacy is determined by audiometric criteria, typically severe to profound sensorineural hearing loss with limited benefit from hearing aids. The criteria vary by country and insurer. An otolaryngologist or cochlear implant center conducts the evaluation.
- Can a cochlear implant make tinnitus worse?
- In a minority of cases, cochlear implant recipients report no change in tinnitus or a worsening of symptoms. This is less common than improvement, but it does occur. Discussing this possibility with the surgical team beforehand is appropriate.
- What happens to tinnitus in the non-implanted ear?
- The tinnitus effect of cochlear implantation is generally specific to the implanted ear. Tinnitus in the contralateral ear is not reliably changed by unilateral implantation.
- Is cochlear implantation ever considered specifically for single-sided deafness and tinnitus?
- Yes. There is a growing body of research on cochlear implantation for single-sided deafness, where one ear has severe to profound loss and the other is normal or near-normal. In this population, tinnitus improvement has been a notable finding in several studies, which has influenced how clinicians consider candidacy.
EarLabs Notes
One short note a week. Tinnitus and hearing health.
New tools, plain-language summaries of recent research, no spam. Unsubscribe in one click.
No tracking pixels, no behavioral retargeting. Read our privacy notes.
Primary sources
- Cochlear Implants — National Institute on Deafness and Other Communication Disorders (NIDCD)
- Cochlear Implants — Mayo Clinic
- Clinical Practice Guideline: Tinnitus — American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS)
- Cochlear Implants — NHS UK