causes
Earwax and tinnitus: when impacted cerumen causes ringing, and safe removal
How impacted earwax can produce conductive tinnitus, why you should never use cotton swabs, and what AAO-HNS recommends instead.
Published May 21, 2026 · By the EarLabs editorial desk
Cerumen, commonly called earwax, is produced by glands in the outer third of the ear canal. It has genuine protective functions: it traps dust and microorganisms, lubricates the canal skin, and possesses mild antimicrobial properties. In most people, the ear canal is self-cleaning. Old cerumen migrates outward as jaw movement and skin migration carry it toward the canal opening.
In some people, cerumen accumulates faster than it exits, or is pushed inward by external objects, and becomes impacted. Impaction is one of the most common and most easily reversible causes of tinnitus.
How earwax produces tinnitus
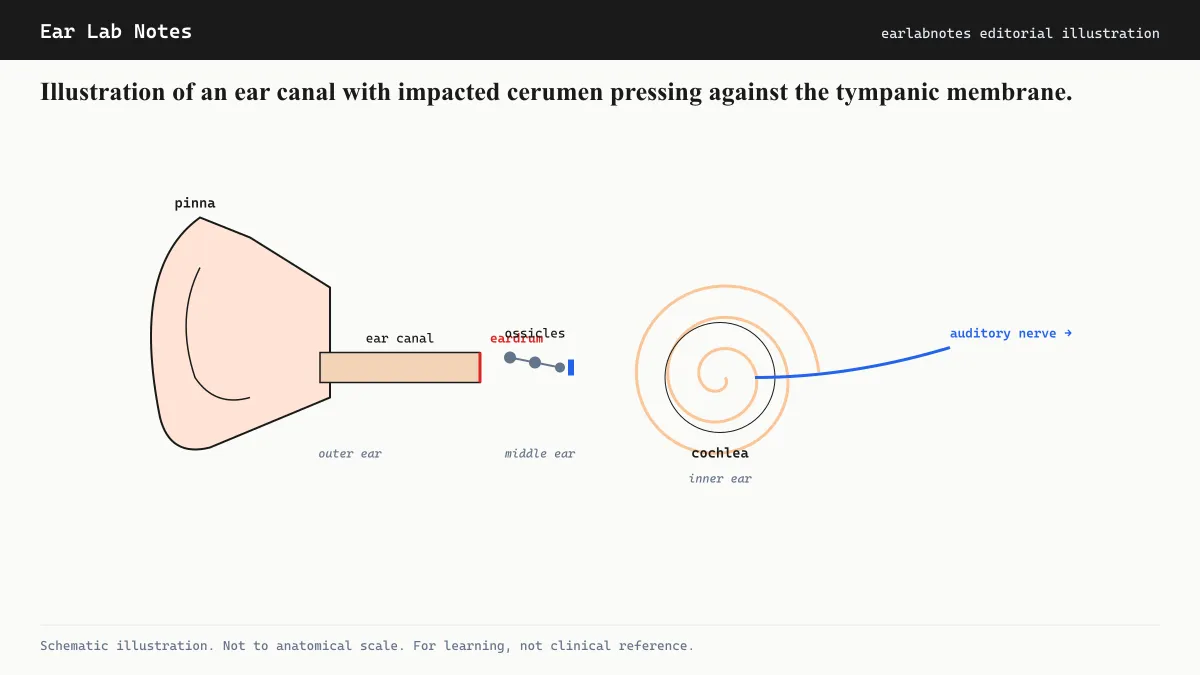
The mechanism is conductive rather than sensorineural. When a plug of cerumen sits against or near the tympanic membrane (eardrum), it can:
Impede sound transmission: Partial or complete blockage of the canal reduces the sound energy reaching the middle and inner ear. The auditory pathway, receiving less input, may respond with compensatory changes that manifest as phantom sound, similar in principle to the central-gain mechanism seen with other forms of hearing reduction.
Create pressure changes: Wax pressing against the eardrum alters its compliance. This can produce a sensation of fullness, muffled hearing, and a low-pitched or variable tinnitus that changes with jaw movement (because the jaw joint shares a wall with the ear canal and its movement shifts cerumen position).
Earwax-induced tinnitus is typically described as low-pitched, muffled, or intermittent rather than the high-pitched ringing associated with noise-induced cochlear damage.
Who is most susceptible to impaction
AAO-HNS identifies several factors that increase cerumen impaction risk:
- Hearing aid use (the device blocks natural cerumen migration and stimulates gland secretion)
- Regular use of cotton swabs or other objects in the canal (the most common patient-driven cause of impaction)
- Narrow or unusually shaped ear canals
- Presence of ear canal hair in older adults
- Use of in-ear earphones or earbuds for prolonged periods
People who wear hearing aids may experience impaction-related tinnitus as a complication of the device even when the device itself is functioning correctly.
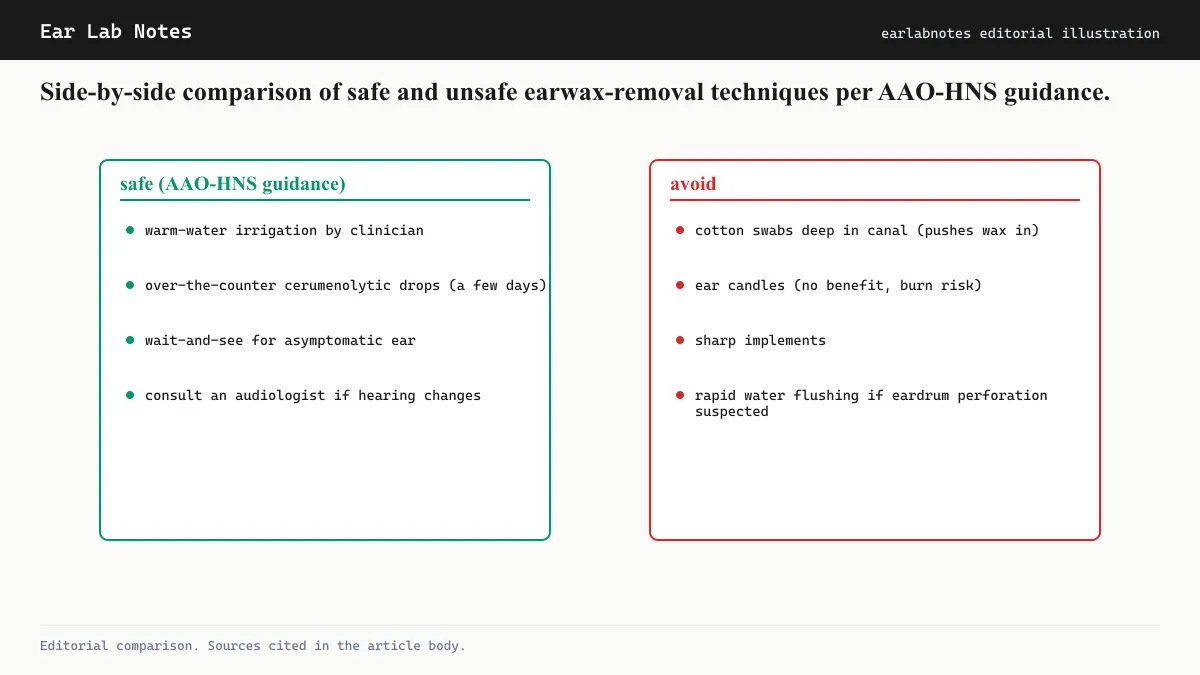
Safe earwax removal: what AAO-HNS recommends
The AAO-HNS published a clinical practice guideline on cerumen impaction. Key points relevant to self-management and clinical removal are:
Self-care options for mild cases
For people without a history of ear surgery, perforated eardrum, or ear tube placement, over-the-counter cerumenolytic (wax-softening) drops such as carbamide peroxide can help soften impacted wax to facilitate natural migration. These are used according to product instructions, typically for several days, and should not be used if any perforation or drainage is suspected.
Irrigation with warm (body-temperature) water, using a soft rubber bulb syringe, is another home approach. Water that is too cold or too warm can cause dizziness by stimulating the vestibular system.
Clinical removal methods
When self-care is insufficient or when impaction is confirmed by examination, a clinician may use:
- Irrigation with a controlled syringe or purpose-built irrigator
- Manual removal with a curette or forceps under direct visualization
- Microsuction, which uses a fine vacuum instrument under magnification and is considered the preferred method in many specialist settings for its precision and reduced risk
All clinical methods carry small risks, primarily minor canal irritation or discomfort, and should only be performed after confirming the eardrum is intact.
What not to do
AAO-HNS guidelines explicitly advise against:
- Inserting cotton swabs, bobby pins, pencils, or any similar object into the ear canal
- Ear candling (hollow candles placed in the canal and lit): no evidence of efficacy, documented injury risk
- Forceful self-irrigation with high-pressure water
What conductive tinnitus sounds like
Clinicians distinguish between conductive tinnitus and sensorineural tinnitus based on the mechanism. Conductive tinnitus arises when sound transmission through the outer or middle ear is impaired. When cerumen blocks the canal, the quiet background sounds that the ear would normally admit from the environment are reduced, and internal sounds such as blood flow, muscle activity, and the body’s own biological noise become relatively louder by comparison.
This is why people with impacted earwax sometimes hear a low or variable hum that worsens in quiet environments and changes when they swallow or move their jaw. It also explains why some people first notice their earwax-related tinnitus after a bath or shower, when water enters the canal and softens or shifts the wax against the eardrum more firmly.
How a clinician confirms cerumen impaction
Diagnosis is made by direct otoscopic examination. A clinician or audiologist looks into the canal with a light and magnification to confirm that wax is present, estimate its extent, and assess whether the eardrum is visible or completely obscured. Attempting to manage tinnitus as if it were cerumen-related without this confirmation is not advisable, because other causes of ear fullness and tinnitus (such as middle ear fluid or eardrum retraction) can produce similar symptoms.
When earwax is not the sole explanation
Tinnitus after cerumen removal that does not resolve suggests another mechanism is contributing. Pre-existing cochlear damage, for example from noise or aging, may have been masked by the conductive component the wax added. Clearing the wax removes the conductive component but leaves the sensorineural tinnitus apparent.
For this reason, audiological assessment after cerumen removal is useful when tinnitus persists. A pure-tone audiogram at that point reflects the underlying cochlear status without the confounding effect of blockage.
Prevention
Since most cerumen impaction is partly driven by inserting objects into the canal, the most effective prevention is also the simplest: stop using cotton swabs inside the ear canal. For people who produce excessive wax or who are prone to impaction due to hearing aid use, periodic professional cleaning on a scheduled basis is a practical approach. An audiologist or otolaryngologist can recommend an appropriate interval based on individual cerumen production.
If symptoms persist or change, see an audiologist or physician.
Frequently asked questions
- Will my tinnitus go away after earwax removal?
- If impacted cerumen is the primary or sole cause of tinnitus, clearing it often resolves or substantially reduces the ringing. However, tinnitus that was present before the impaction developed, or that has additional causes, may persist after removal. An audiologist or clinician can assess this after the wax is cleared.
- Is ear candling a safe way to remove earwax?
- No. AAO-HNS and other clinical bodies advise against ear candling. There is no evidence it removes cerumen effectively, and it carries documented risks including burns to the face and ear canal, occlusion of the canal with candle debris, and perforation of the eardrum.
- How do I know if I have impacted earwax?
- Common signs include a sensation of fullness or blockage in the ear, muffled hearing, tinnitus, and occasionally mild discomfort or itching. A clinician can confirm impaction by direct examination of the ear canal with an otoscope. Self-diagnosis is unreliable.
- Are cotton swabs safe for ear hygiene?
- AAO-HNS guidance advises against inserting cotton swabs or any other objects into the ear canal. The outer ear (the shell visible from outside) can be cleaned gently with a cloth, but the canal itself is largely self-cleaning. Swabs push wax deeper rather than removing it, which is a common cause of impaction.
EarLabs Notes
One short note a week. Tinnitus and hearing health.
New tools, plain-language summaries of recent research, no spam. Unsubscribe in one click.
No tracking pixels, no behavioral retargeting. Read our privacy notes.
Primary sources
- Clinical Practice Guideline: Cerumen Impaction - AAO-HNS — American Academy of Otolaryngology, Head and Neck Surgery
- Tinnitus - NIDCD — National Institute on Deafness and Other Communication Disorders
- Earwax - NHS — NHS UK
- Tinnitus - Mayo Clinic — Mayo Clinic