science
Hidden hearing loss: when an audiogram looks normal but listening is hard
Cochlear synaptopathy damages the synapses between hair cells and auditory neurons before audiometric thresholds shift. Why this matters for tinnitus and what 'normal' audiograms miss.
Published May 21, 2026 · By the EarLabs editorial desk
The gap between how you hear and what the audiogram shows
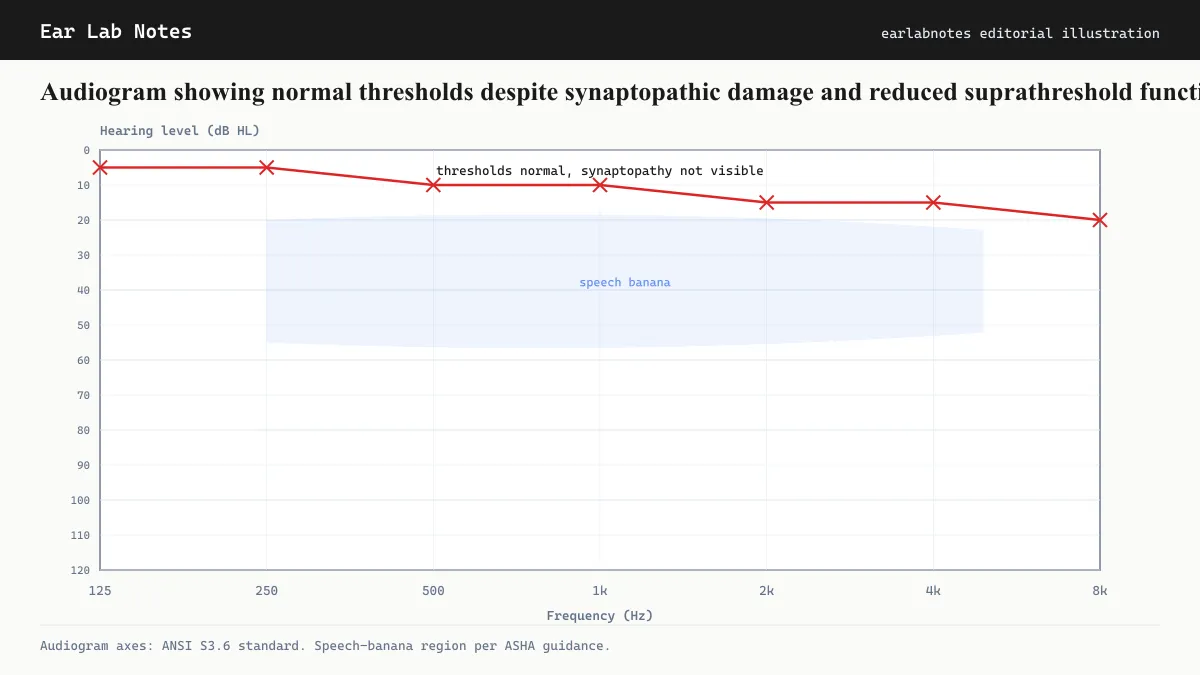
An audiogram measures one thing: the softest sound you can detect at each tested frequency. It is an excellent test for what it measures. It identifies whether hearing thresholds are within normal limits, and if not, how much they deviate from normal and at which frequencies.
What it does not measure is how many auditory nerve fibers are carrying signals. A person can lose a substantial fraction of their auditory nerve synapses while retaining enough functional connections to detect threshold-level tones. The audiogram looks normal. But the auditory system is working with reduced capacity, and certain demanding tasks, particularly following speech in noise, become noticeably harder.
This is cochlear synaptopathy, sometimes called hidden hearing loss.
The ribbon synapse and its role
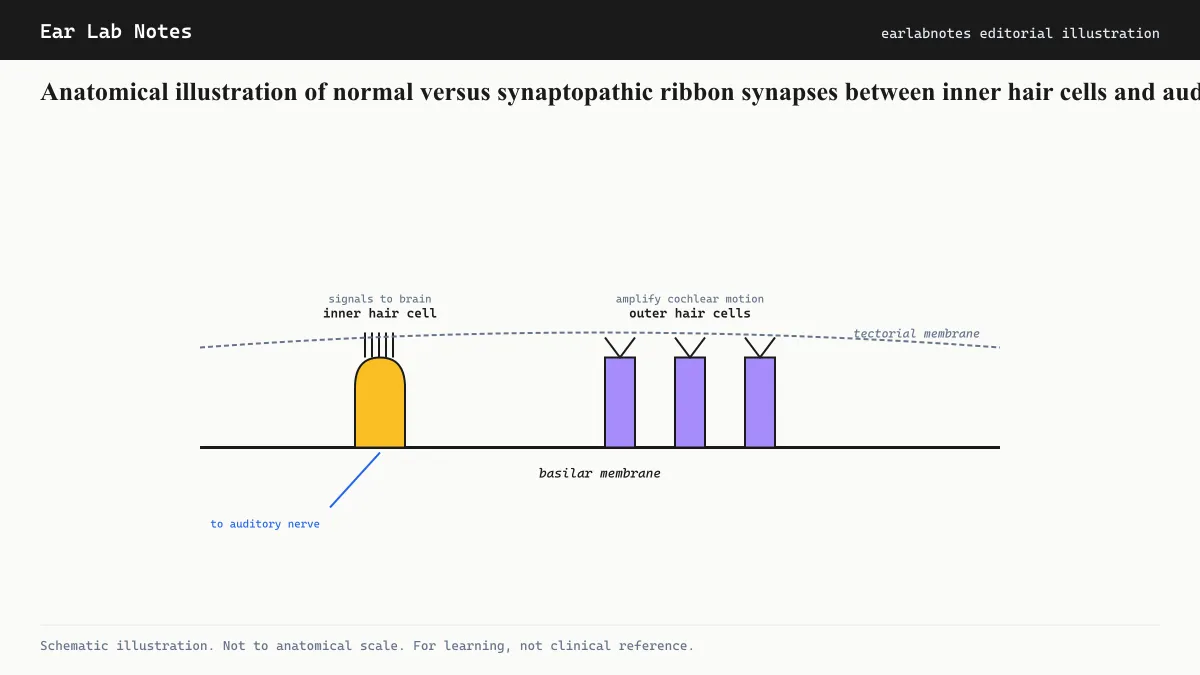
Inner hair cells in the cochlea connect to auditory nerve fibers at specialized junctions called ribbon synapses. The ribbon synapse is an unusually capable structure. It sustains rapid, continuous neurotransmitter release in response to sound, allowing auditory nerve fibers to follow the fine temporal structure of sounds at rates far higher than most other synapses in the body.
A single inner hair cell makes contact with multiple auditory nerve fibers. Those fibers are not identical: some have high spontaneous firing rates and low acoustic thresholds (they respond to very quiet sounds), while others have low spontaneous rates and high thresholds (they respond only to louder sounds). The high-threshold, low-spontaneous-rate fibers appear to be selectively vulnerable to noise-induced damage.
This selective vulnerability is important for understanding why hidden hearing loss is hidden. Standard threshold audiometry depends on detecting soft sounds, which is the job of high-spontaneous-rate, low-threshold fibers. These fibers are relatively resistant to the noise damage that kills ribbon synapses. The vulnerable high-threshold fibers contribute to suprathreshold hearing (hearing sounds clearly above the detection threshold, particularly in complex listening environments). Losing them does not shift detection thresholds but reduces the richness of what the auditory nerve can encode.
How the concept emerged
Animal research, initially in mice and guinea pigs, established that acoustic exposures which produce only temporary threshold shifts (the temporary muffling after a loud concert, which resolves overnight) can nonetheless cause permanent, irreversible loss of ribbon synapses. The hair cells survived; the connections did not.
Subsequent work extrapolated this to humans using post-mortem cochlear tissue and inferred it from electrophysiological measurements in living subjects. Research groups funded through NIDCD programs documented that the number of auditory nerve synapses per inner hair cell declines with age and accelerates with noise exposure history, even in ears with audiometrically normal thresholds.
The term “hidden hearing loss” was coined to describe this discordance, but the formal scientific term is cochlear synaptopathy.
Why the audiogram misses it
The audiogram’s blind spot comes from what it is designed to detect. Threshold detection is a task that requires only minimal neural resources. Even with significant synapse loss, enough fibers remain to detect a quiet tone in silence. The test passes.
The task that reveals synaptopathy is different: understanding speech in noise requires the auditory nerve to encode the precise timing and level differences that separate a target voice from background noise. This is a suprathreshold task. It demands high temporal precision and a large population of functioning nerve fibers to encode the subtle cues that distinguish speech from noise.
When auditory nerve fiber count is reduced, even if thresholds are normal, the signal-to-noise encoding capacity of the nerve is reduced. Speech in noise becomes harder to follow. Background sounds that were once manageable become masking problems. This is the symptom pattern most consistently associated with cochlear synaptopathy.
Tests that can detect what audiograms miss
Standard audiograms are insufficient for detecting synaptopathy. Research settings use supplementary measurements:
Electrocochleography (ECochG) measures electrical potentials generated by the hair cells and auditory nerve in response to sound. The summing potential (SP) and action potential (AP) amplitudes, and their ratio, reflect the neural output of the cochlea in ways that threshold audiometry does not.
Auditory brainstem response (ABR) at high sound levels can measure the total neural output of the auditory nerve. Reduced wave I amplitude of the ABR relative to later brainstem-generated waves suggests peripheral synaptopathy.
Speech-in-noise testing, such as the QuickSIN or HINT, assesses the real-world functional consequence of synaptopathy, though it does not directly measure the synapses. Normal audiogram paired with significantly reduced speech-in-noise performance is a clinical pattern consistent with hidden hearing loss.
These tests are not yet part of routine audiological workup for most patients, but awareness of synaptopathy is growing, and specialist audiologists increasingly include suprathreshold testing when patients report difficulty in noise with normal thresholds.
The tinnitus connection
Cochlear synaptopathy may help explain a population that has puzzled tinnitus researchers: people with tinnitus and apparently normal audiograms. The central-gain hypothesis predicts that when peripheral input is reduced, the central auditory pathway increases its gain. Synaptopathy reduces auditory nerve fiber count and therefore total neural input, even if threshold-level signals can still get through.
NIDCD-affiliated researchers have proposed that this reduced input, invisible to the audiogram, may nonetheless be sufficient to drive central gain upward. The amplified internal neural noise would then be perceptible as tinnitus. Animal evidence supports this: synaptopathic mice show evidence of elevated central auditory gain and tinnitus-related behaviors.
If this model is correct, it suggests that people who have ringing ears and a normal audiogram are not imagining their tinnitus. They may have a form of cochlear damage that standard testing cannot detect.
Prevention remains the same
Whether the target of concern is threshold elevation or synaptopathy, the prevention advice is the same. Noise exposure at levels and durations above NIOSH guidelines damages the cochlea. The synaptopathy model suggests the damage may occur at lower cumulative doses than previously understood, because temporary threshold shifts (which were once considered reassuring evidence of reversible effects) are now associated with permanent synapse loss.
Hearing protection, limiting music volume through headphones, and avoiding prolonged exposure to loud recreational environments are the measures with evidence behind them.
If symptoms persist or change, see an audiologist or physician.
Frequently asked questions
- What is hidden hearing loss?
- Hidden hearing loss refers to cochlear synaptopathy, damage to the synaptic connections between inner hair cells and auditory nerve fibers. It is called 'hidden' because standard audiometric threshold testing does not detect it. Thresholds remain in the normal range even as the auditory nerve loses some of its carrying capacity.
- What symptoms does hidden hearing loss cause?
- The most consistent symptom is difficulty understanding speech in noisy environments, sometimes described as needing conversations to be quieter or needing speakers to slow down. People with synaptopathy often pass standard hearing tests and are told their hearing is normal, which can be frustrating when the subjective difficulty is real.
- Is hidden hearing loss permanent?
- Cochlear synaptopathy from noise exposure appears to be largely permanent in mammals, based on animal research. Synapses that are lost following acute noise trauma do not spontaneously regenerate. Whether very gradual, low-level damage over decades differs in its reversibility is an area of active research.
- Can hidden hearing loss cause tinnitus?
- NIDCD-affiliated researchers have proposed that cochlear synaptopathy may contribute to tinnitus in people with apparently normal audiograms. If enough auditory nerve fibers are lost, the central auditory pathway may compensate by increasing gain, and that gain can amplify internal noise into perceived ringing.
- How is cochlear synaptopathy diagnosed?
- There is no routine clinical test for synaptopathy in humans. Research methods include electrocochleography and auditory brainstem response (ABR) measurements, which can detect reduced neural output below what threshold audiograms capture. These tests are more commonly found in research settings than standard audiology clinics.
EarLabs Notes
One short note a week. Tinnitus and hearing health.
New tools, plain-language summaries of recent research, no spam. Unsubscribe in one click.
No tracking pixels, no behavioral retargeting. Read our privacy notes.
Primary sources
- Noise-Induced Hearing Loss — NIH/NIDCD
- Tinnitus: Overview and Management — NIH/NIDCD
- Hearing Loss — NHS UK
- Hearing Loss: Diagnosis and Treatment — Mayo Clinic