types
Hyperacusis vs tinnitus: when ordinary sounds become painfully loud
Hyperacusis is sound intolerance, tinnitus is phantom sound. They share central-gain mechanisms and often co-occur. How clinicians distinguish them.
Published May 21, 2026 · By the EarLabs editorial desk
Tinnitus and hyperacusis are related, but they are not the same thing. Tinnitus is the perception of a sound that has no external source: ringing, buzzing, hissing, or clicking that only you can hear. Hyperacusis is a reduced tolerance for ordinary environmental sounds that most people find comfortable or even quiet.
A person with hyperacusis may find a normal conversation painful. Traffic, cutlery on plates, or a ringing telephone can cross a discomfort threshold that sits far below where most people feel anything at all.
Both conditions are real, both are measurable, and both can be distressing. Understanding the difference matters because their mechanisms overlap in some ways but diverge in others, and that shapes how clinicians approach each one.
What hyperacusis actually is
The word comes from Greek: hyper (over) and akousis (hearing). The formal clinical definition is a significantly reduced tolerance for sound in the presence of normal or near-normal audiometric thresholds.
Crucially, hyperacusis is not the same as a simple dislike of noise. It is a physiological change in how the auditory system processes volume. Sounds that register as comfortable for most listeners register as intolerably loud, uncomfortable, or even painful for someone with hyperacusis.
The NIDCD (National Institute on Deafness and Other Communication Disorders) notes that hyperacusis can occur alongside hearing loss, tinnitus, or independently. Exact prevalence is hard to pin down because definitions vary, but surveys suggest it affects a meaningful minority of adults.
How clinicians measure it
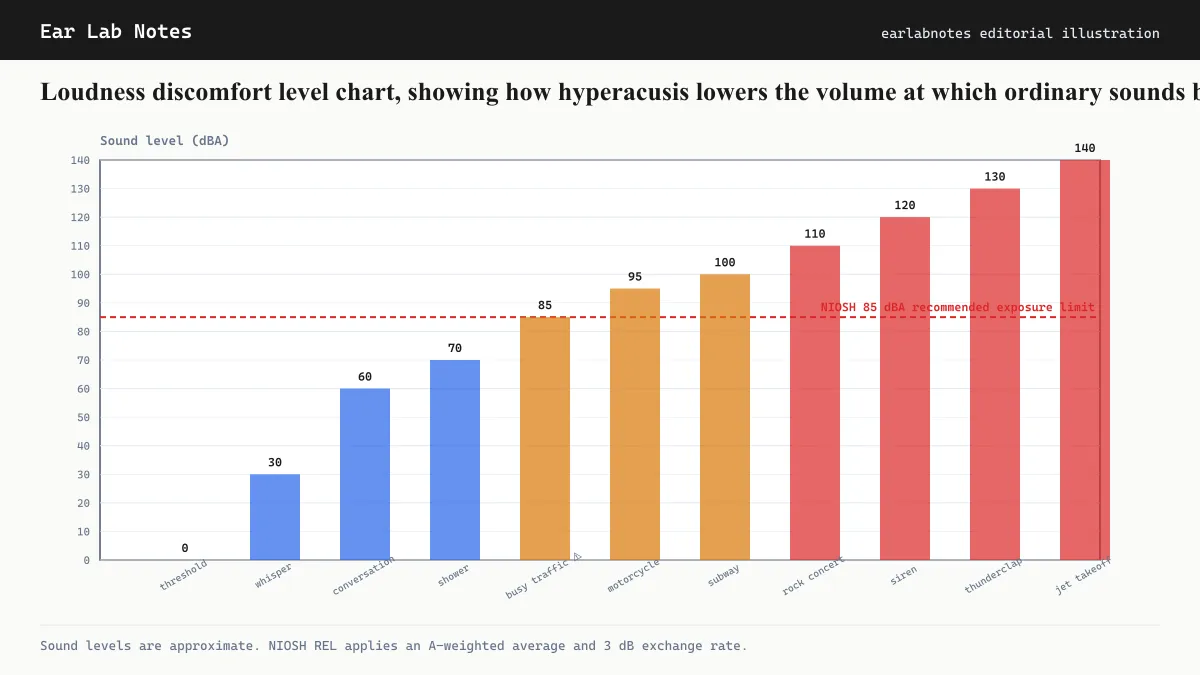
The standard measurement is the loudness discomfort level (LDL) test. An audiologist presents tones at increasing volumes and asks the patient to indicate when the sound becomes uncomfortable. In people without hyperacusis, discomfort typically begins somewhere above 90 dB-HL. In hyperacusis, that threshold can fall to 60, 50, or even lower.
A full evaluation usually includes a standard pure-tone audiogram, speech recognition testing, and LDL measurements across multiple frequencies.
The central-gain connection
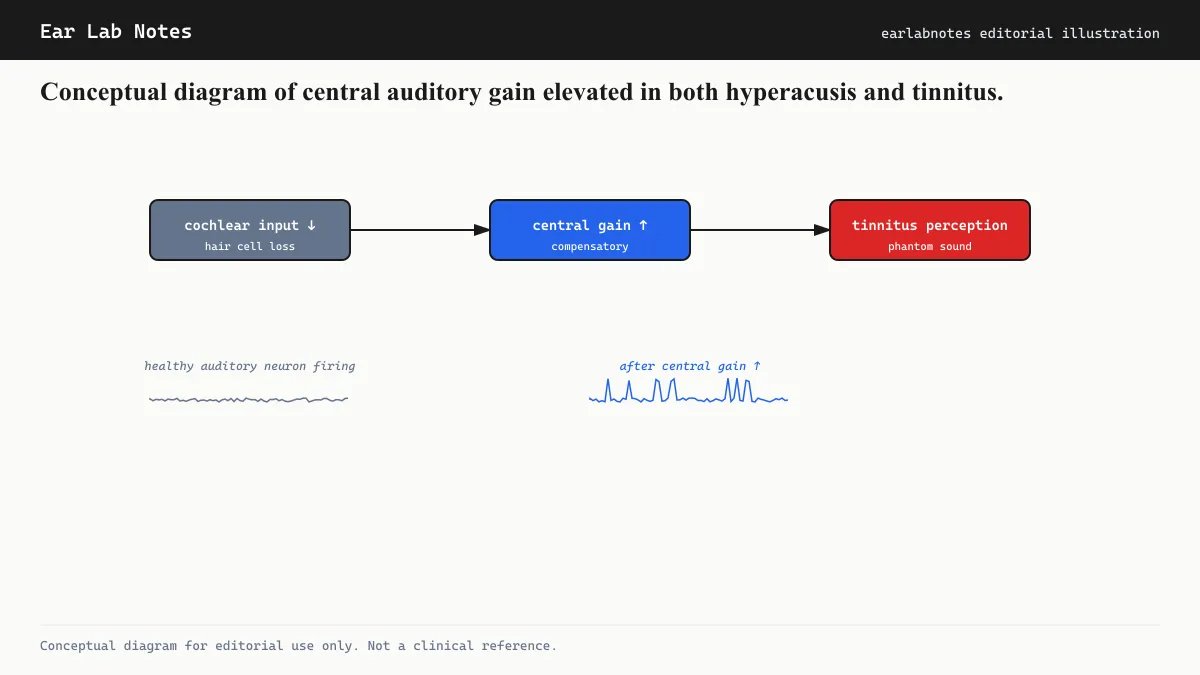
To understand why tinnitus and hyperacusis so often appear together, it helps to understand the concept of central auditory gain.
When the cochlea sends fewer signals to the brain, perhaps because of noise damage or aging, the auditory brain compensates by turning up its internal amplification. Researchers often compare this to turning up the volume on a stereo when the signal from the source weakens. The amplified signal makes soft sounds perceptible, which is useful. But it also amplifies the system’s own internal noise, which may be perceived as tinnitus. And it can make moderate external sounds feel disproportionately loud, which is hyperacusis.
This shared mechanism helps explain why the two conditions co-occur at rates far above chance. Research surveys, cited in reviews published through NIDCD and the British Tinnitus Association (BTA), suggest that somewhere between 40 and 86 percent of people with hyperacusis also experience tinnitus.
Key differences between the two
Despite their shared mechanisms, tinnitus and hyperacusis are distinct clinical entities.
Source of the experience. Tinnitus is a phantom sound: it comes from inside the auditory system with no external stimulus. Hyperacusis is an abnormal response to real external sounds.
Measurement. Tinnitus is evaluated through pitch matching and loudness matching. Hyperacusis is evaluated through LDL testing.
Triggers. Tinnitus can occur in complete silence. Hyperacusis requires an external sound to be present.
Primary distress. Tinnitus distress often relates to anxiety about the sound, intrusion during concentration, and sleep disruption. Hyperacusis distress often relates to anticipatory fear of sound, avoidance of social situations, and physical discomfort or pain.
Conditions that can cause or worsen both
Several conditions are associated with both hyperacusis and tinnitus. Noise-induced hearing damage is among the most common. Other associated conditions include:
- Lyme disease (in some cases)
- Bell’s palsy (via the stapedius reflex nerve)
- Williams syndrome (a genetic condition)
- Post-traumatic stress following acoustic trauma
- Certain autoimmune inner ear conditions
Migraines are also associated with temporary sound sensitivity, though migraine-related photophobia and phonophobia are considered distinct from true hyperacusis.
Management approaches
The AAO-HNS (American Academy of Otolaryngology) and the BTA both emphasize that management of hyperacusis requires individualized assessment. No single approach works for everyone, and the evidence base is still developing.
Sound therapy and desensitization
Clinicians often use a gradual sound exposure protocol, sometimes called sound desensitization therapy. The goal is to gently re-acclimate the auditory system to everyday sounds without triggering pain. This is typically delivered through an audiologist or hearing therapist and progresses slowly over weeks or months.
Patients are generally advised against wearing earplugs in quiet or moderately loud everyday environments, because prolonged sound deprivation can make central gain even higher and worsen sensitivity over time. Ear protection is still appropriate in genuinely hazardous noise levels.
Psychological support
The BTA and NHS UK both note that psychological components of hyperacusis, particularly anticipatory anxiety and avoidance behavior, can maintain and worsen the condition independently of the auditory mechanism. Cognitive behavioral approaches, similar to those used for tinnitus, address these patterns.
For co-occurring tinnitus
When both conditions are present, treatment planning typically addresses both. Sound enrichment strategies used in tinnitus management (low-level background sound, sound generators) may also reduce the jarring contrast that makes hyperacusis worse. An audiologist experienced with both conditions is best placed to coordinate a combined approach.
What to expect from an evaluation
A thorough evaluation for hyperacusis involves more than a standard hearing test. Look for a provider who performs LDL testing across multiple frequencies, takes a detailed history of sound exposure and symptom onset, and screens for co-occurring tinnitus and anxiety. The NIDCD recommends evaluation by a specialist in auditory disorders when sound sensitivity is affecting daily life.
If symptoms persist or change, see an audiologist or physician.
Frequently asked questions
- Can you have both hyperacusis and tinnitus at the same time?
- Yes. Research surveys suggest somewhere between 40 and 86 percent of people with hyperacusis also report tinnitus. Both conditions appear to involve elevated central auditory gain, so their co-occurrence is not surprising. A full audiological evaluation can assess both simultaneously.
- Is hyperacusis permanent?
- Outcomes vary considerably. Some people experience improvement, particularly when the onset is linked to a temporary cause such as a middle-ear infection. Others find the condition persists. Clinicians generally advise against both overprotection with earplugs in quiet settings and overexposure to loud noise, as either extreme can make the condition worse. Consult an audiologist for an individualized assessment.
- What is the difference between hyperacusis and misophonia?
- Hyperacusis is a broadly reduced tolerance for sound across many frequencies and volumes. Misophonia is a strong aversive reaction to specific trigger sounds (often chewing or breathing) regardless of their loudness. The two can overlap but are clinically distinct. An audiologist or psychologist with experience in auditory conditions can help differentiate them.
- Does wearing earplugs in quiet environments help hyperacusis?
- Evidence suggests that routinely wearing earplugs in quiet or moderately loud environments can worsen hyperacusis over time by making the auditory system even more sensitive. Earplugs are generally appropriate for genuinely damaging sound levels. For everyday noise, clinicians typically favor a gradual, guided sound exposure approach. Discuss this with an audiologist before making changes.
EarLabs Notes
One short note a week. Tinnitus and hearing health.
New tools, plain-language summaries of recent research, no spam. Unsubscribe in one click.
No tracking pixels, no behavioral retargeting. Read our privacy notes.
Primary sources
- Hyperacusis (Sound Sensitivity) — NIH/NIDCD
- Tinnitus Clinical Practice Guideline — American Academy of Otolaryngology - Head and Neck Surgery (AAO-HNS)
- Hyperacusis — NHS Inform (Scotland)
- Tinnitus and Hyperacusis — British Tinnitus Association (BTA)