frequencies
Low-frequency tinnitus: when ringing sounds more like a hum or roar
Low-pitched tinnitus is less common than high-pitched but is the signature of Meniere's disease, eustachian tube dysfunction, and some vascular causes.
Published May 21, 2026 · By the EarLabs editorial desk
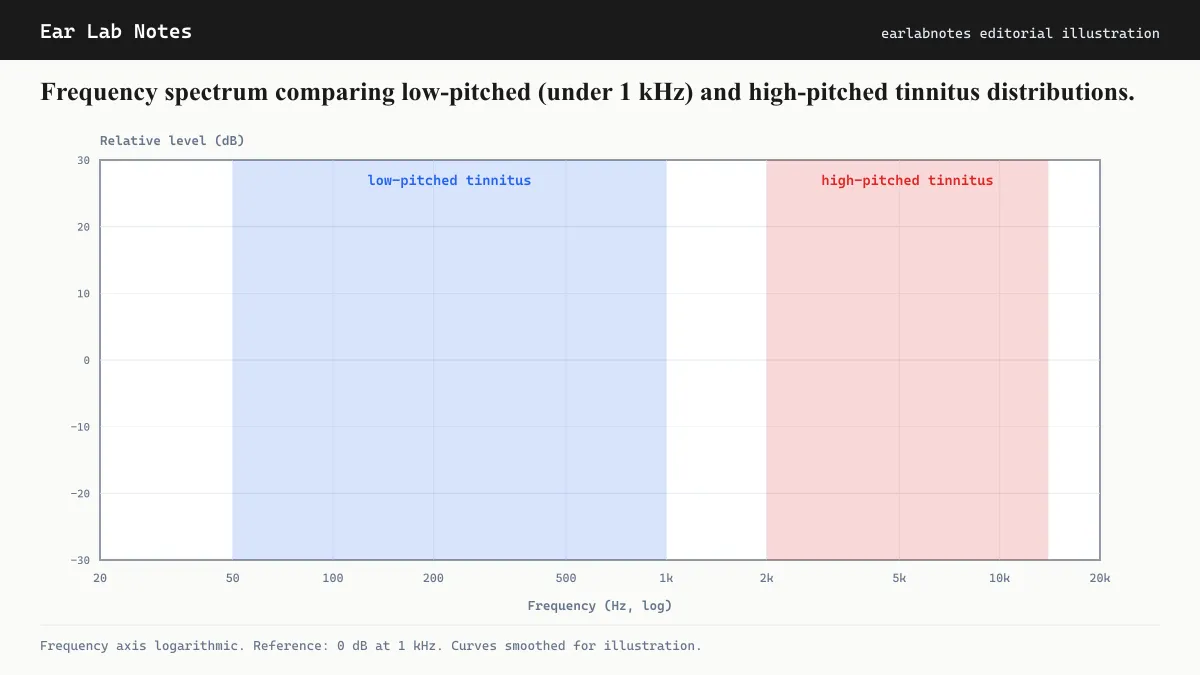
Tinnitus is most commonly described as high-pitched: a ringing, hissing, or whistling tone. But a substantial minority of people with tinnitus describe something quite different. Their tinnitus sits in the low end of the audible range, between about 100 Hz and 1,000 Hz. They describe it as a hum, a roar, a drone, or a rumble that can sound almost like a machine running somewhere nearby.
Low-frequency tinnitus is clinically meaningful because it is rarer than high-frequency tinnitus, is associated with a somewhat different set of underlying causes, and can require a different evaluation approach.
Why low-frequency tinnitus is less common
The most prevalent cause of tinnitus generally is cochlear hair cell damage from noise exposure and aging, both of which hit the high-frequency basal cochlea preferentially. This makes high-frequency tinnitus the statistically dominant pattern.
Low-frequency tinnitus requires either damage or dysfunction in the apical (low-frequency) portion of the cochlea, or a mechanism that bypasses cochlear tonotopy entirely. These situations are less common, which explains the lower prevalence.
The main causes of low-frequency tinnitus
Meniere’s disease
Meniere’s disease is the condition most closely associated with low-frequency tinnitus. The NIDCD describes it as an inner ear disorder characterized by four classic features: episodic vertigo, fluctuating hearing loss, ear fullness (aural fullness), and tinnitus.
The tinnitus of Meniere’s is characteristically low-pitched, described as roaring, rumbling, or a low hum. It typically fluctuates, becoming louder or more prominent in the period before a vertigo episode and sometimes quieting between attacks.
The underlying mechanism involves endolymphatic hydrops, an accumulation of the fluid endolymph in the inner ear’s membranous labyrinth. This increased fluid pressure is thought to distort the mechanics of the apical (low-frequency) cochlea, producing the characteristic low-pitched sensorineural hearing loss and the associated low-pitched tinnitus.
The Mayo Clinic notes that low-frequency sensorineural hearing loss is considered one of the diagnostic criteria for Meniere’s disease, and it is this hearing loss pattern that correlates with the low-frequency tinnitus pitch.
Eustachian tube dysfunction
The eustachian tube connects the middle ear to the back of the throat and equalizes air pressure on both sides of the eardrum. When it does not function properly, pressure imbalance in the middle ear can produce hearing changes, ear fullness, and sometimes low-frequency tinnitus.
This tinnitus is typically conductive in nature: it results from altered sound transmission through the middle ear rather than from cochlear or neural dysfunction. When eustachian tube function is restored (by treatment of underlying causes like allergies, congestion, or reflux), the tinnitus often resolves.
Vascular causes
Pulsatile tinnitus, which beats in synchrony with the heartbeat, is sometimes perceived as a low-frequency rhythmic sound rather than a steady tone. Large venous structures near the ear, including the jugular vein and its branches, can produce low-frequency vascular sounds that are transmitted to the cochlea.
Superior semicircular canal dehiscence, a thinning or absence of bone over one of the semicircular canals, can also produce low-frequency conductive hearing effects and associated tinnitus.
Somatic and mechanical causes
Patulous eustachian tube, a condition where the tube remains abnormally open instead of closed, can produce low-frequency hearing of one’s own voice and breathing (autophony) and sometimes tinnitus. This is distinct from eustachian tube dysfunction, where the tube is blocked.
Some cervicogenic (neck-related) somatic tinnitus cases present as low-frequency sounds, particularly when large muscles of the neck are involved.
Audiometric patterns in low-frequency tinnitus
Standard audiograms test from 250 Hz to 8,000 Hz. In Meniere’s disease, the audiogram typically shows a low-frequency sensorineural hearing loss pattern, with the worst thresholds at 250 and 500 Hz and relatively better thresholds at higher frequencies. This inverted pattern is the opposite of the high-frequency notch seen in noise-induced hearing loss.
In conductive causes (eustachian tube dysfunction, middle-ear fluid), the audiogram may show a conductive hearing loss, where air-conduction thresholds are worse than bone-conduction thresholds.
Audiologists may also perform electrocochleography (ECochG), a test that measures the electrical response of the cochlea to sound and can provide evidence of endolymphatic hydrops when Meniere’s disease is suspected.
Management considerations
The management of low-frequency tinnitus depends substantially on its cause.
For Meniere’s disease, management focuses on the underlying condition. Dietary sodium restriction is a common first-line recommendation. The rationale is that reducing sodium intake may decrease endolymphatic fluid pressure. The evidence base for specific treatments in Meniere’s is reviewed by the AAO-HNS and the NIDCD, which both note that the condition follows an unpredictable course and that no single intervention is universally effective.
For conductive causes (eustachian tube dysfunction, middle-ear fluid), treating the underlying condition, whether allergies, sinusitis, or reflux contributing to tube dysfunction, can resolve the tinnitus.
For vascular pulsatile low-frequency tinnitus, imaging is the first step. The AAO-HNS notes that pulsatile tinnitus warrants evaluation to identify any treatable vascular abnormality.
Standard tinnitus management approaches, including sound therapy, counseling, and CBT, can also be applied to low-frequency tinnitus. Matching the masking or enrichment sound to the low-frequency range of the tinnitus may be more effective than using standard broadband sounds.
If symptoms persist or change, see an audiologist or physician.
Frequently asked questions
- What does low-frequency tinnitus sound like?
- People with low-frequency tinnitus typically describe it as a hum, roar, rumble, or drone rather than a ringing or high-pitched whine. Some describe it as similar to an engine running in the distance, or a persistent low vibration. The sound is often fluctuating rather than steady, particularly when Meniere's disease is involved.
- Is low-frequency tinnitus harder to treat than high-frequency tinnitus?
- The evidence base for tinnitus management does not clearly distinguish treatment effectiveness by pitch. However, because low-frequency tinnitus is more often associated with identifiable underlying conditions (such as Meniere's disease or eustachian tube dysfunction), addressing the underlying condition can sometimes reduce or alter the tinnitus. Consult an audiologist and otolaryngologist for an individual assessment.
- Can the Hum (as reported in some news stories) be a form of low-frequency tinnitus?
- Some researchers have suggested that cases of the so-called Hum, where individuals report hearing a persistent low-frequency drone without an identifiable external source, may involve tinnitus in some cases. However, the phenomenon is incompletely understood. If you are experiencing new persistent low-frequency sounds, audiological evaluation can help determine whether a tinnitus mechanism is involved.
- How is low-frequency tinnitus evaluated?
- Evaluation typically includes a full audiogram with extended low-frequency testing, electrocochleography (which can detect endolymphatic hydrops), and otoscopy. If pulsatile features are present, vascular imaging may be added. The specific tests depend on the clinical presentation and which conditions are suspected.
EarLabs Notes
One short note a week. Tinnitus and hearing health.
New tools, plain-language summaries of recent research, no spam. Unsubscribe in one click.
No tracking pixels, no behavioral retargeting. Read our privacy notes.
Primary sources
- Meniere's Disease — NIH/NIDCD
- Tinnitus — NIH/NIDCD
- Meniere's Disease — Mayo Clinic
- Tinnitus: causes and management — NHS UK