types
Subjective vs objective tinnitus: which 1% can a doctor actually hear
Why nearly all tinnitus is subjective (only you hear it), what the rare objective forms sound like to a clinician, and how the distinction changes the workup.
Published May 21, 2026 · By the EarLabs editorial desk
When someone says they have tinnitus, almost invariably they are describing a sound that only they can hear. No instrument held up to their ear would detect it; it is generated inside the auditory nervous system, not by a physical sound source inside the body. This is called subjective tinnitus, and it represents roughly 99 percent of all tinnitus cases.
A rare but clinically distinct form, objective tinnitus, is different: the sound has an actual physical source inside the body, and in some cases a clinician using a stethoscope or sensitive microphone can detect it from outside. Understanding the difference between these two categories changes how tinnitus is investigated and managed.
Defining subjective tinnitus
Subjective tinnitus is the perception of sound in the absence of an external acoustic stimulus, without a physical sound source inside the body that could be measured externally. The sound is generated by aberrant activity in the auditory pathway, whether at the level of the cochlea, the auditory nerve, the brainstem relay nuclei, or the auditory cortex.
The underlying mechanisms include cochlear hair cell damage, maladaptive central gain increases, somatosensory input to the dorsal cochlear nucleus, and others. All of these produce phantom sound that only the person experiencing it perceives.
Subjective tinnitus can be:
- Continuous or intermittent
- High-pitched or low-pitched
- Unilateral (one ear) or bilateral
- Constant in quality or variable
NIDCD, Mayo Clinic, and NHS UK all describe subjective tinnitus as the dominant form of the condition. The AAO-HNS clinical practice guideline on tinnitus is written primarily with subjective primary tinnitus in mind.
Defining objective tinnitus
Objective tinnitus has a real acoustic source inside the body. The sound can be detected or recorded externally under the right conditions. There are three main categories.
Pulsatile vascular tinnitus
This is the most common form of objective tinnitus. Turbulent blood flow in vessels near the ear, from conditions including carotid stenosis, arteriovenous malformations, high blood pressure, or a high-riding jugular bulb, generates sound that is transmitted through bone and tissue to the cochlea. A clinician listening with a stethoscope placed over the mastoid bone or the neck may detect the same bruit the patient hears.
Pulsatile vascular tinnitus is synchronized with the heartbeat and has the character of a rhythmic whooshing or thumping.
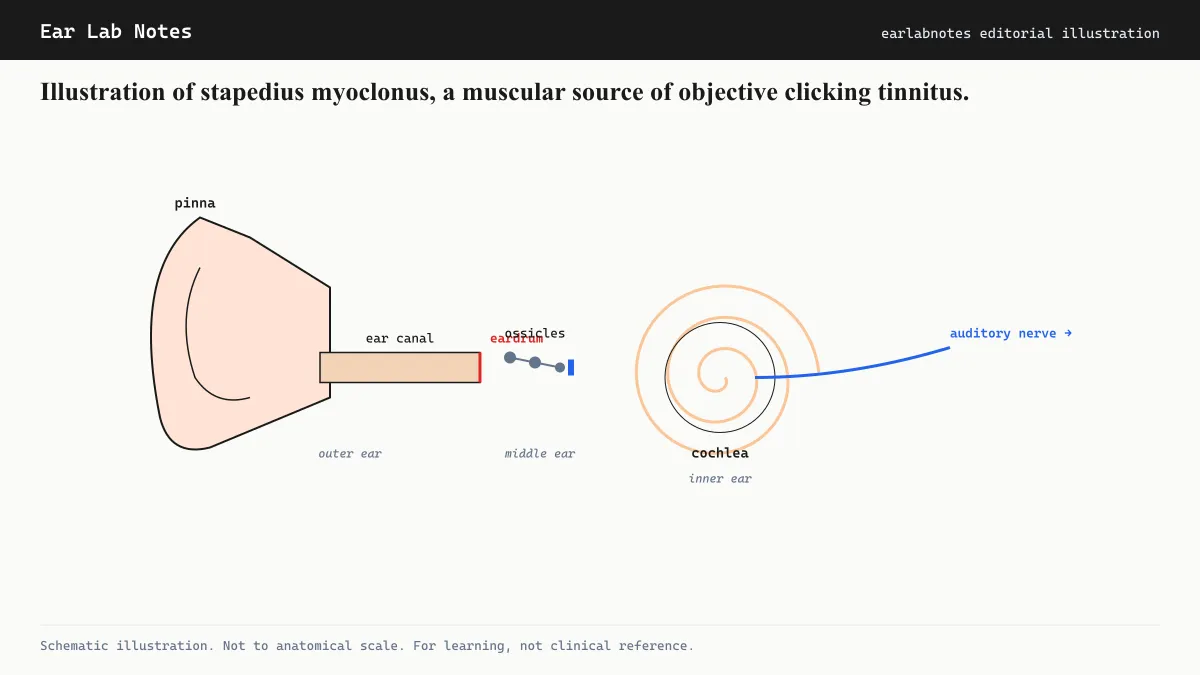
Middle ear myoclonus
The middle ear contains two small muscles: the stapedius (attached to the stapes, one of the ossicles) and the tensor tympani (attached to the malleus). Normally these muscles contract briefly in response to loud sound as part of the acoustic reflex. In myoclonus, they contract rhythmically and involuntarily at rest, producing clicking or crackling sounds that are transmitted through the ossicular chain to the cochlea and perceived as tinnitus.
In some cases, a trained examiner can hear these clicks without instruments by placing an ear close to the external canal. A sensitive microphone or tympanometry equipment can record the movement. The condition is typically intermittent and may worsen with fatigue or anxiety.
Palatal myoclonus
Rhythmic contractions of the palatal muscles, particularly the levator veli palatini and tensor veli palatini, can open and close the eustachian tube repetitively, producing a clicking sound perceived in the ear. These contractions may be visible to a clinician examining the soft palate, making palatal myoclonus one of the more reliably confirmable forms of objective tinnitus.
Palatal myoclonus can be essential (without identifiable cause) or symptomatic (associated with brainstem lesions), and the clinical evaluation differs accordingly.
Patulous eustachian tube: a related phenomenon
A closely related condition is a patulous (abnormally open) eustachian tube. Normally the eustachian tube is closed at rest and opens briefly during swallowing or yawning to equalize pressure. When it remains open, the patient hears their own breathing and voice resonating in the ear (called autophony) as well as heartbeat sounds. This is not strictly tinnitus because the sounds have real sources (the patient’s own voice and cardiopulmonary sounds), but it is often grouped clinically with the objective forms because it involves a detectable physical mechanism.
How the distinction changes clinical workup
The most important practical consequence of distinguishing subjective from objective tinnitus is in directing investigation.
For subjective tinnitus, the evaluation focuses on the auditory system: audiogram, imaging if red flags are present (asymmetric tinnitus, focal neurological symptoms), and assessment for correctable causes (earwax, medication review, blood pressure).
For objective or suspected-objective tinnitus, additional steps become relevant: auscultation of the neck and periauricular region, vascular imaging (CT angiography or MRI angiography) to assess for vascular anomalies, tympanometry to assess middle ear compliance, and referral to neurotology or neurology depending on findings.
The treatment implications also differ sharply. Vascular objective tinnitus may be amenable to endovascular or surgical intervention. Myoclonus-related tinnitus may respond to treatment of an underlying trigger or, in some cases, Botox injection or surgical myotomy. Subjective tinnitus has no equivalent structural target and is managed through audiological and psychological approaches.
Diagnostic techniques for suspected objective tinnitus
When a clinician suspects an objective cause, the evaluation uses specific techniques that go beyond the standard audiogram:
Auscultation: Placing a stethoscope over the mastoid bone (behind the ear), the periauricular region, and the lateral neck allows the clinician to listen for bruits that correspond to what the patient hears. Some vascular pulsatile tinnitus is reliably detectable in this way.
Tympanometry and acoustic reflex testing: Middle ear myoclonus may produce measurable artifact in tympanometric recordings, where the probe-tone signal fluctuates rhythmically as the middle ear muscles contract. This can provide objective corroboration of the patient’s subjective description.
High-resolution otoscopy: For palatal myoclonus, visual inspection of the soft palate during the episode may reveal rhythmic muscular contractions visible from the oral cavity.
Microphone recording: A sensitive probe microphone placed in the external ear canal can sometimes record the objective tinnitus signal directly, providing a recording that can be analyzed spectrally. This is more commonly used in research settings but is technically feasible in specialist clinics.
Imaging: CT of the temporal bone without contrast evaluates bony anatomy including the jugular bulb, carotid canal, and middle ear space. CTA or MRA of the head and neck assesses vascular structures. These are ordered based on the specific objective form suspected.
How patients can help clinicians distinguish the types
Several observations a patient can make at home are useful to report during a clinical evaluation:
Whether the tinnitus follows the heartbeat, whether it changes when swallowing (relevant to palatal myoclonus and eustachian tube function), whether it changes with head position or pressure on the neck, whether it is intermittent or continuous, and whether it is present in one or both ears. These details substantially narrow the differential before any examination is performed.
Why objective tinnitus matters despite its rarity
Even though objective tinnitus represents a small minority of cases, clinicians ask about the character of tinnitus specifically because pulsatile quality is a red flag that changes the workup significantly. AAO-HNS guidelines specifically call out pulsatile tinnitus as a condition warranting imaging consideration. Missing a treatable vascular cause by failing to ask whether the tinnitus beats with the pulse is a meaningful clinical error.
For the large majority of people with subjective tinnitus, the distinction is reassuring: their tinnitus does not indicate a vascular anomaly or muscular dysfunction requiring specialized intervention.
If symptoms persist or change, see an audiologist or physician.
Frequently asked questions
- If my doctor can't hear my tinnitus with a stethoscope, does that mean nothing is wrong?
- No. The vast majority of tinnitus, estimated at around 99 percent, is subjective and cannot be heard by anyone else. The inability of a clinician to hear it externally is entirely normal and does not suggest the sound is imagined or insignificant. Subjective tinnitus can cause substantial distress and warrants evaluation and management regardless.
- What does middle ear myoclonus sound like?
- Middle ear myoclonus (rapid rhythmic contractions of the stapedius or tensor tympani muscles) typically produces clicking or crackling sounds. Some people describe it as the sound of a butterfly wing or a light clicking. It tends to occur in bursts and may be associated with stress, fatigue, or caffeine. In some cases a clinician can record the sound with a sensitive microphone placed in the canal.
- Is patulous eustachian tube serious?
- Patulous eustachian tube is not typically dangerous, but it can be quite bothersome. The symptom of autophony (hearing your own voice resonating loudly in your ear) is distinctive. Management options exist and are usually conservative. An otolaryngologist familiar with eustachian tube dysfunction can evaluate and advise.
- Can objective tinnitus be cured?
- Some causes of objective tinnitus are directly treatable. Pulsatile tinnitus from a dural arteriovenous fistula can often be resolved with endovascular treatment. Middle ear myoclonus sometimes responds to treatment of an underlying trigger. The prognosis depends entirely on the specific underlying cause, which requires evaluation to identify.
EarLabs Notes
One short note a week. Tinnitus and hearing health.
New tools, plain-language summaries of recent research, no spam. Unsubscribe in one click.
No tracking pixels, no behavioral retargeting. Read our privacy notes.
Primary sources
- Tinnitus - NIDCD — National Institute on Deafness and Other Communication Disorders
- Tinnitus - Mayo Clinic — Mayo Clinic
- Clinical Practice Guideline: Tinnitus - AAO-HNS — American Academy of Otolaryngology, Head and Neck Surgery
- Tinnitus - NHS — NHS UK