management
Tinnitus and sleep: why nights are worst and how to break the cycle
Sleep deprivation worsens tinnitus and tinnitus worsens sleep. Cognitive, environmental, and behavioral interventions with the strongest evidence for breaking the feedback loop.
Published May 21, 2026 · By the EarLabs editorial desk
Night is reliably the hardest part of the day for many people with chronic tinnitus. Clinicians who work in this field hear it consistently: the ringing that was manageable during a busy workday becomes the loudest thing in the room once the lights go off and the house goes quiet.
Understanding why this happens, and what interventions have the strongest evidence for addressing it, is useful for anyone navigating tinnitus management.
Why tinnitus intensifies at night
The explanation has two parts, one acoustic and one cognitive.
On the acoustic side, bedrooms are quieter than most daytime environments. The background noise floor drops significantly. Since tinnitus is a phantom sound that stands out most clearly against silence, the reduction in environmental noise makes the ringing more perceptible. It is not that the tinnitus is louder; it is that the contrast is greater.
On the cognitive side, people going to sleep are no longer engaged in tasks that occupy attention. During the day, work, conversation, and activity compete for cognitive resources. At night, that competition disappears and attention naturally drifts toward the most salient stimulus in the environment. For someone with tinnitus, that stimulus is often the ringing itself.
The bidirectional feedback loop
Sleep and tinnitus are linked in both directions. Tinnitus disrupts sleep, and sleep disruption worsens tinnitus. Research summarized by NIDCD and discussed in Mayo Clinic patient resources points to this bidirectional relationship as a central feature of chronic tinnitus management.
When sleep is poor, cognitive arousal increases, the limbic system becomes more reactive, and the auditory system’s sensitivity appears to rise. The result is that tinnitus feels more intrusive on days after poor sleep, which can create anxiety about bedtime, which in turn makes sleep harder. The cycle can become self-reinforcing relatively quickly.
Breaking the loop usually requires addressing both components: the sleep environment and the cognitive response to tinnitus.
Environmental strategies: sound enrichment
The most straightforward intervention is reducing the contrast between silence and tinnitus by adding background sound. This is called sound enrichment in BTA guidance.
Options include dedicated white noise machines, fan noise, pink or brown noise from a smartphone app, or quiet ambient music. The specific sound matters less than whether it is pleasant enough to tolerate and consistent enough not to create its own distractions.
BTA guidance on sound enrichment recommends keeping the masking sound below the tinnitus level, known as partial masking, so that the tinnitus is mixed with rather than completely covered by the background. The reasoning is that prolonged total masking delays the habituation process that many management programs aim to support.
Volume matters for safety as well. Prolonged exposure to sound above 70 dBA at close range can itself contribute to hearing damage, according to NIOSH standards. A bedside device kept at a comfortable conversational level is well within safe parameters.
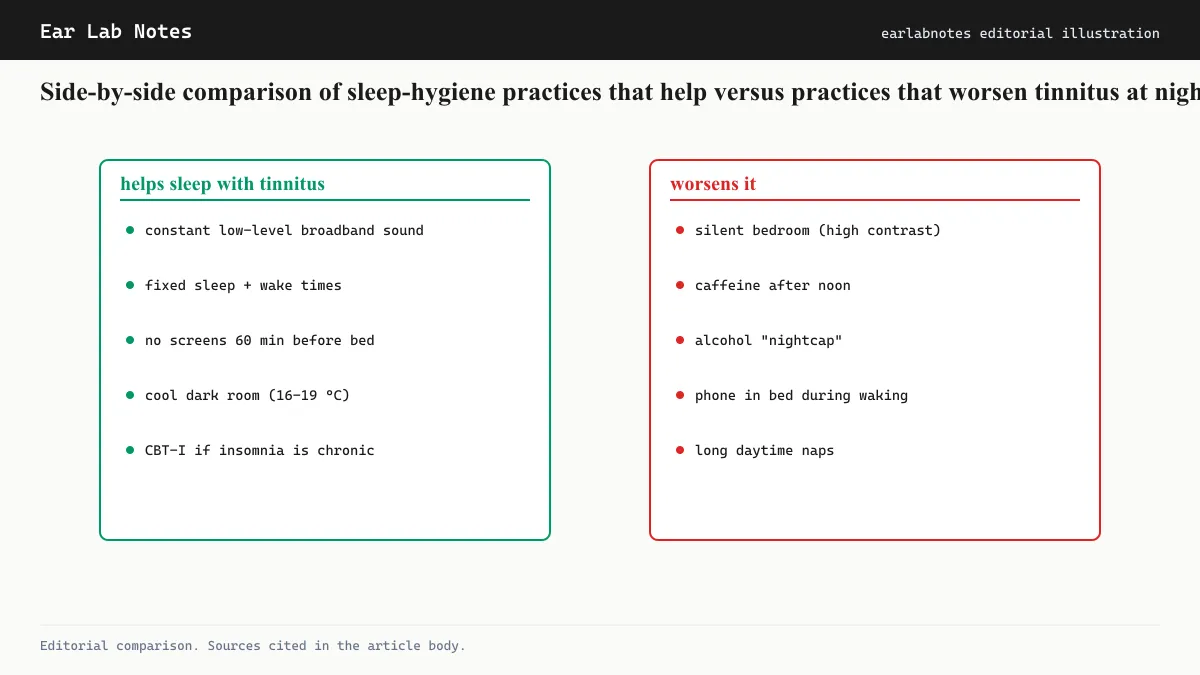
Behavioral strategies: sleep hygiene
Sleep hygiene is a set of behavioral practices designed to strengthen the association between bed and sleep while reducing factors that increase arousal at bedtime. They apply to insomnia generally, and tinnitus research incorporates them as a component of management programs.
Consistent sleep and wake times stabilize circadian rhythm, which is one of the most robust predictors of sleep quality across the medical literature. Irregular schedules fragment the rhythm and make falling asleep harder.
Avoiding screens in the final hour before sleep reduces light-based circadian disruption. Avoiding alcohol is relevant because, while alcohol initially promotes drowsiness, it fragments sleep architecture in the second half of the night, which is when tinnitus is often most disruptive.
Keeping the bedroom cool and dark reduces the arousal signals that compete with the onset of sleep. Temperature regulation is among the better-established factors in sleep-onset research.
Cognitive activation before bed
One of the most common patterns in people with tinnitus-related insomnia is a cycle of negative thinking at bedtime. Thoughts such as “I will not be able to sleep because of the ringing” activate the arousal system, which makes sleep harder, which confirms the prediction. Cognitive behavioral therapy for insomnia (CBT-I) addresses this cycle directly.
CBT-I is distinct from CBT for tinnitus, though the two overlap substantially. Both involve restructuring unhelpful thought patterns. CBT-I specifically targets the cognitive and behavioral factors that perpetuate insomnia. Research reviewed by NIDCD indicates it is effective for insomnia in the general population, and smaller studies have examined its application in tinnitus populations with encouraging results.
Relaxation techniques before sleep
Relaxation techniques reduce physiological arousal and shift attention away from the tinnitus signal. Progressive muscle relaxation, controlled breathing, and body-scan practices have all appeared in tinnitus management programs.
These are not cures for tinnitus or insomnia. They are tools for lowering the baseline level of nervous system activation at bedtime, which makes both sleep onset and the perception of tinnitus slightly more manageable. The NHS includes relaxation as part of its general tinnitus self-management guidance.
Medications and sleep
Some people with tinnitus and insomnia ask about sleep medications. This is a conversation for a physician rather than an editorial publication. What is worth noting from an informational standpoint is that sedating antihistamines and benzodiazepines can affect sleep architecture in ways that may not address the underlying insomnia, and some medications that affect the central nervous system have complex relationships with tinnitus.
Any discussion of sleep medication in the context of tinnitus warrants a conversation with a clinician who is aware of the full medical picture.
When to seek professional help
Sleep disruption that persists beyond two to three weeks despite behavioral changes, or that significantly affects daytime function, is generally considered a reason to seek professional evaluation. A physician can assess whether there are comorbid sleep disorders such as sleep apnea, which has its own relationship with tinnitus, and whether referral to a sleep specialist or audiologist is appropriate.
The AAO-HNS clinical practice guideline on tinnitus specifically identifies comorbid sleep disturbance as a factor that should prompt more comprehensive management rather than watchful waiting.
If symptoms persist or change, see an audiologist or physician.
Frequently asked questions
- Why does tinnitus seem louder at night?
- The bedroom environment is typically quieter than daytime settings. With less competing sound, the contrast between silence and the phantom tinnitus signal is larger, making the ringing more perceptible. There is also less cognitive distraction from tasks, which directs more attention toward the sound.
- Can sleep deprivation actually make tinnitus worse?
- Research reported in the literature associated with NIDCD and Mayo Clinic suggests that sleep deprivation increases the perception of tinnitus loudness and distress. The relationship appears bidirectional: poor sleep amplifies tinnitus salience, and tinnitus disrupts sleep.
- Is it safe to use a white noise machine all night?
- At moderate volumes, yes. Guidance from the BTA and NIOSH both caution against prolonged exposure above roughly 70 dBA. A white noise machine set to a comfortable level, well below the hearing-damage threshold, is generally considered safe for overnight use.
- Should I avoid silence completely?
- Many audiologists and BTA guidance recommend sound enrichment, keeping the environment from being completely silent, as a practical strategy for tinnitus management. Whether that means a dedicated device, a fan, or quiet music is a matter of preference.
- Does treating sleep problems help tinnitus?
- There is evidence that improving sleep quality reduces tinnitus distress. CBT for insomnia, which is different from CBT for tinnitus but overlapping in technique, has been studied in this population and shows positive effects on both sleep and tinnitus-related distress in some trials.
EarLabs Notes
One short note a week. Tinnitus and hearing health.
New tools, plain-language summaries of recent research, no spam. Unsubscribe in one click.
No tracking pixels, no behavioral retargeting. Read our privacy notes.
Primary sources
- Tinnitus — National Institute on Deafness and Other Communication Disorders (NIDCD)
- Tinnitus: Diagnosis and Treatment — Mayo Clinic
- Tinnitus — NHS UK
- Sleep and Tinnitus — British Tinnitus Association (BTA)
- Clinical Practice Guideline: Tinnitus — American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS)