management
Tinnitus retraining therapy (TRT): what it is and how long it takes
TRT combines counseling and low-level broadband sound to habituate the auditory system to tinnitus. Treatment timeline, evidence, and how it differs from CBT and masking.
Published May 21, 2026 · By the EarLabs editorial desk
Tinnitus retraining therapy, widely known by its acronym TRT, is a structured long-term approach to reducing tinnitus-related distress and habituating the auditory and emotional systems to the tinnitus signal. It was developed by audiologist Pawel Jastreboff and refined through work at the University of Maryland and subsequent institutions in the 1990s.
TRT is not a cure. Its goal is habituation: the process by which the auditory brain learns to classify the tinnitus signal as unimportant, eventually routing it away from conscious awareness much as people stop noticing the hum of a refrigerator or air conditioning unit.
The approach combines two components: directive counseling and sound therapy. Each addresses a different aspect of how tinnitus generates distress.
The neurophysiological model
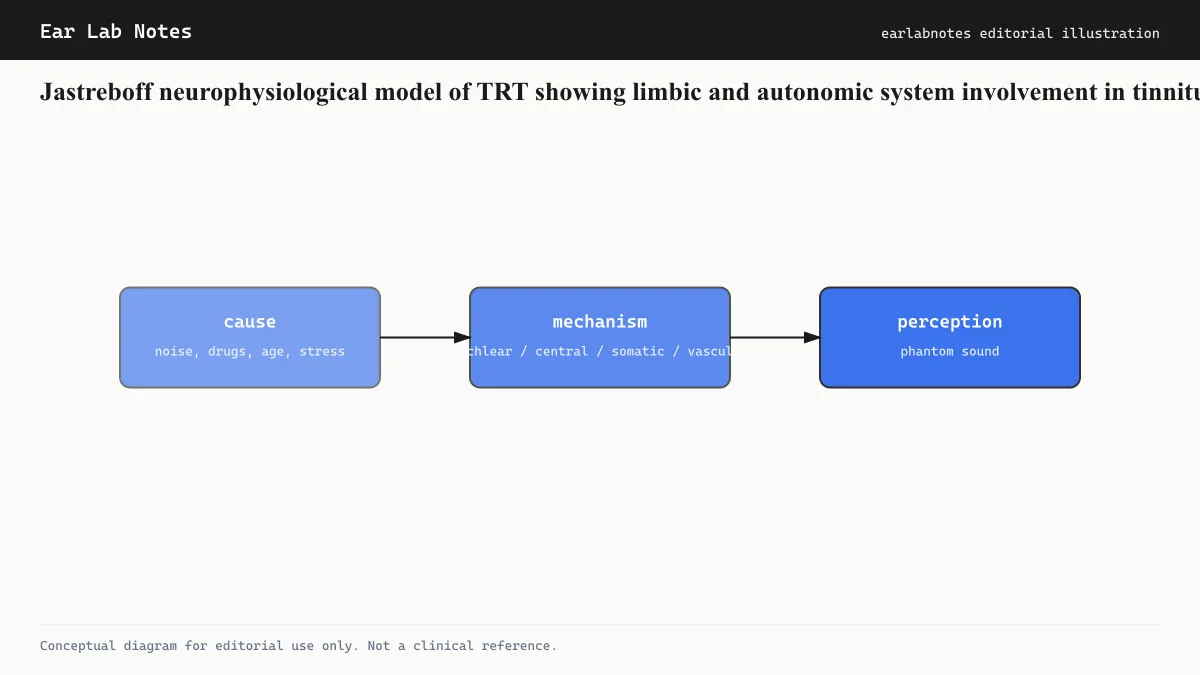
TRT is grounded in a specific model of how tinnitus becomes distressing. The Jastreboff neurophysiological model proposes that tinnitus becomes a problem not simply because of the auditory signal itself, but because of connections between the auditory system and two other brain systems: the limbic system (emotion) and the autonomic nervous system (stress responses).
In this model, the tinnitus signal becomes distressing when the limbic system classifies it as threatening. Once that classification is made, the autonomic system generates a stress response, negative emotions become conditioned to the sound, and attention is automatically drawn to it. This conditioned response maintains the distress and prevents habituation from occurring naturally.
TRT’s directive counseling targets the limbic classification: by changing the meaning assigned to the tinnitus signal, it removes the emotional charge that keeps the tinnitus prominent. Sound therapy supports this by ensuring the auditory system is not deprived of stimulation, which keeps the brain from over-amplifying the tinnitus.
Directive counseling
The counseling component of TRT is called directive because it follows a structured educational approach rather than open-ended talking therapy.
A TRT clinician walks the patient through the neurophysiological model, explains how tinnitus is generated, and makes the case that the tinnitus is not dangerous and not a sign of serious neurological disease (assuming this has been established through appropriate medical evaluation). The explicit goal is to demystify the tinnitus and reduce the fear and negative significance attached to it.
This is not dismissing the patient’s experience. The distress is real. The counseling reframes the source of the distress, locating it in the brain’s learned response to the signal rather than in the signal itself. This reframing is what opens the door to habituation.
Sessions typically address common misconceptions: that tinnitus always gets worse with time, that it inevitably destroys quality of life, or that nothing can be done. Each of these beliefs, when held, makes habituation harder.
Sound therapy in TRT
The sound therapy component of TRT is distinctive and frequently misunderstood. It is not masking.
Masking aims to cover the tinnitus completely by using a louder competing sound, making the tinnitus inaudible. TRT explicitly avoids this. Instead, it uses sound generators set below the level of the tinnitus, so that both the environmental sound and the tinnitus are audible simultaneously.
The principle is that the auditory brain learns to habituate to sounds that are consistently present at low levels and carry no negative significance. By surrounding the tinnitus with low-level neutral sound, and simultaneously removing the negative emotional association through counseling, the brain can begin to process the tinnitus as background rather than foreground.
TRT patients typically wear behind-the-ear sound generators (similar in appearance to hearing aids) for extended periods daily. The protocol often specifies six to eight hours of wear per day. The sound level is set during clinical appointments and adjusted over the course of treatment.
For patients with coexisting hearing loss, combination instruments (devices that function as both hearing aids and sound generators) may be used.
The treatment timeline
TRT is a long-term commitment. Unlike some interventions that show effects within weeks, TRT typically requires 12 to 18 months for full habituation to develop.
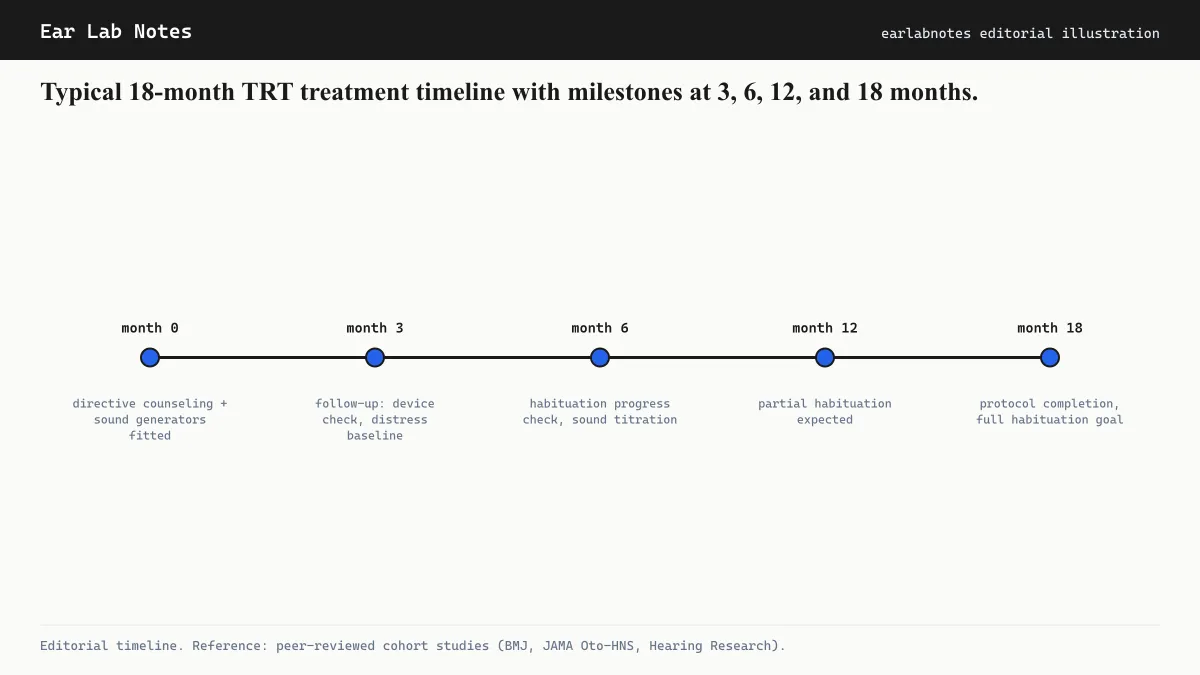
A typical treatment arc follows a general pattern:
Months 0 to 3: Initial counseling sessions establish the therapeutic framework. Sound generators are fitted and calibrated. Patients learn the neurophysiological model and begin daily wear. Reduction in distress may begin but is often gradual.
Months 3 to 6: Many patients report initial improvements in sleep, anxiety, and the intrusiveness of the tinnitus during this period, though results vary considerably between individuals.
Months 6 to 12: Continued counseling and sound generator use. Habituate responses deepen for many patients.
Months 12 to 18: Some patients move toward reducing sound-generator use as habituation becomes more robust. Follow-up appointments assess progress and adjust the protocol.
This timeline is general and individual variation is substantial. Some patients progress more quickly; others find the process takes longer.
How TRT compares to other approaches
TRT versus masking
Traditional tinnitus masking uses sound to cover the tinnitus, providing relief while the masker is on but not targeting the underlying habituation process. TRT uses sound specifically to support habituation, not to provide temporary cover. The mechanisms are different, and TRT proponents argue that complete masking can actually slow habituation by preventing the brain from processing and reclassifying the tinnitus signal.
TRT versus CBT
CBT for tinnitus and TRT both involve counseling but differ in their theoretical foundation and method. CBT targets cognitive and behavioral patterns (thoughts, avoidance, attention). TRT targets the neurophysiological response through prolonged low-level sound exposure and directive educational counseling. Both have evidence supporting their effectiveness, and some programs combine elements of each. The Mayo Clinic and NIDCD both list TRT and CBT as structured options for chronic tinnitus.
Patient categories in TRT
The original TRT protocol defined patient categories based on the severity and type of tinnitus, the presence of hearing loss, and the presence of hyperacusis. The protocol is adjusted by category: patients with hyperacusis, for example, follow a modified sound-therapy approach that begins with very low sound levels and progresses carefully to avoid worsening sound sensitivity.
Identifying which category applies requires clinical assessment by a TRT-trained audiologist.
If symptoms persist or change, see an audiologist or physician.
Frequently asked questions
- How is TRT different from CBT for tinnitus?
- Both involve counseling, but TRT is grounded in the Jastreboff neurophysiological model, which emphasizes auditory system habituation through prolonged low-level sound exposure combined with directive counseling. CBT focuses on changing thoughts, emotional responses, and behaviors related to tinnitus. TRT uses sound generators more systematically than most CBT protocols. Some clinicians combine elements of both. A specialist can advise which approach may be more suitable for a given presentation.
- What is directive counseling in TRT?
- Directive counseling in TRT is a structured educational component that explains the neurophysiological model of tinnitus to the patient, reframes the tinnitus as a non-threatening signal, and reduces fear-based responses. The goal is to remove the emotional significance attached to the tinnitus so that the auditory system's habituation mechanisms can operate. It is called directive because the counselor leads the patient through a specific conceptual framework rather than using open-ended talking therapy.
- Do I need to wear sound generators all day?
- TRT protocol typically involves wearing sound generators for extended periods each day (often 6 to 8 hours or more), not for masking but to maintain a low level of background sound that facilitates habituation. The settings are kept below the tinnitus level so that the tinnitus remains audible. This is a key difference from masking. The exact protocol varies by clinician and patient category. Follow the guidance of the TRT specialist you work with.
- Is TRT covered by insurance?
- Coverage varies by country, insurer, and healthcare system. In the UK, TRT is available through some NHS audiology services. In the US, coverage through health insurance is inconsistent. An audiologist or ENT specialist can advise on what is available in your area.
- Is there good evidence that TRT works?
- TRT has been studied in controlled trials and observational series. Results generally show improvements in tinnitus distress, though the evidence base has limitations including small sample sizes and varying outcome measures across studies. The NIDCD notes TRT as one of the structured approaches for chronic tinnitus management. It has not been shown to be consistently superior to other evidence-based approaches, and individual responses vary.
EarLabs Notes
One short note a week. Tinnitus and hearing health.
New tools, plain-language summaries of recent research, no spam. Unsubscribe in one click.
No tracking pixels, no behavioral retargeting. Read our privacy notes.
Primary sources
- Tinnitus — NIH/NIDCD
- Clinical Practice Guideline: Tinnitus — American Academy of Otolaryngology - Head and Neck Surgery (AAO-HNS)
- Tinnitus — Mayo Clinic
- Tinnitus Retraining Therapy — British Tinnitus Association (BTA)