causes
TMJ disorders and tinnitus: how the jaw joint produces ear ringing
Anatomical and somatic links between the temporomandibular joint and the middle ear, why TMJ-related tinnitus often changes when you move your jaw, and standard management approaches.
Published May 21, 2026 · By the EarLabs editorial desk
The temporomandibular joint (TMJ) is the hinge that connects the lower jaw to the skull, just in front of each ear. Disorders of this joint and the surrounding muscles are known collectively as temporomandibular disorders (TMD). One of the less immediately obvious consequences of TMD is tinnitus, a connection that puzzles many people because the jaw and ear seem like unrelated structures. The anatomical proximity and shared developmental origins of the jaw joint and middle ear explain how jaw dysfunction can produce phantom ear sounds.
Why the jaw and ear are anatomically linked
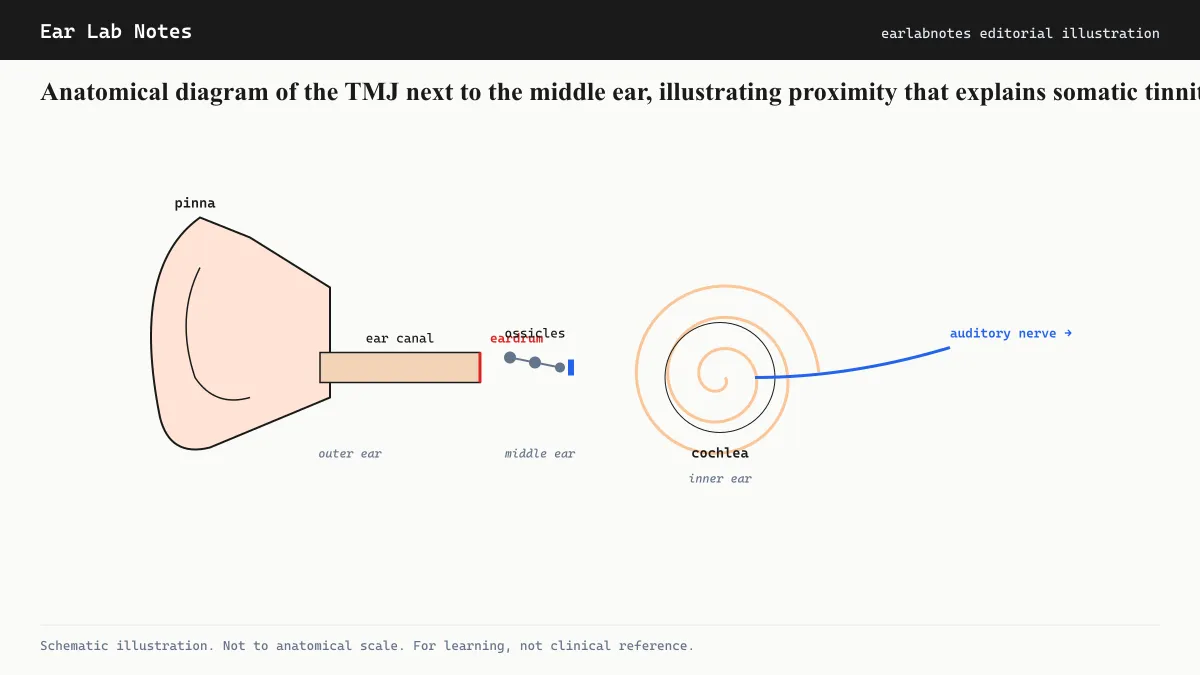
The TMJ sits in a small depression in the temporal bone called the glenoid (or mandibular) fossa. This hollow is separated from the ear canal by only a thin bony plate. During jaw movements, the condyle of the mandible moves within the fossa, and because this motion occurs directly adjacent to the ear canal and the tympanic membrane, it can transmit mechanical sensations into the auditory system.
Beyond proximity, there is a deeper developmental connection. Several of the small bones of the middle ear, particularly the malleus and incus, evolved from jaw bones shared with distant reptilian ancestors. A small ligament called the discomalleolar ligament connects the articular disc of the TMJ directly to the malleus, one of the three ossicles responsible for transmitting sound from the eardrum to the inner ear. Dysfunction or displacement of the TMJ disc can exert mechanical stress through this ligament directly onto the middle ear ossicles.
The somatosensory pathway
Beyond mechanical coupling, TMJ-related tinnitus operates through a neural mechanism. The dorsal cochlear nucleus, a brainstem relay station in the auditory pathway, receives two types of input: auditory signals from the cochlea and somatosensory signals from the trigeminal nerve, which innervates the jaw, face, and TMJ region.
Under normal circumstances, these two inputs are balanced. When somatosensory input is abnormal, as it can be when the jaw muscles are in chronic spasm or when TMJ joint mechanics are disrupted, the dorsal cochlear nucleus receives an aberrant signal that it generates into phantom auditory activity. This is the mechanism of somatic tinnitus.
A clinically useful feature of somatic tinnitus is that it can often be modulated by the patient: changing jaw position, pressing on specific jaw muscles, or moving the neck can temporarily alter the pitch or loudness of the tinnitus. This is called somatic modulation, and its presence is one marker that somatosensory pathways are involved.
TMD as a recognized tinnitus cause
NIDCD lists jaw joint and muscle problems (TMD) among the recognized causes of tinnitus. The relationship is bidirectional in some cases: tinnitus-related distress can increase jaw clenching and teeth grinding (bruxism), which in turn worsens TMJ loading.
The prevalence of tinnitus among people with diagnosed TMD is substantially higher than in the general population in multiple published studies, though the direction of causation in any individual case requires clinical assessment.
Recognizing TMJ-related tinnitus
Features that may point toward a TMJ contribution include:
- Tinnitus that began around the time of jaw injury, dental work, or changes in bite alignment
- Jaw pain, clicking, or limited opening ability alongside tinnitus
- Tinnitus that is louder in the morning (consistent with nocturnal bruxism)
- Tinnitus that changes when the jaw is opened wide, clenched, or moved side to side
- Tinnitus accompanied by facial pain, headaches, or neck tension
None of these features are diagnostic by themselves, but their presence should prompt evaluation of the jaw joint as part of the tinnitus assessment.
Standard management approaches
Management of TMJ-related tinnitus typically addresses the jaw component and the tinnitus component in parallel. Clinical approaches for the jaw component may include:
Occlusal splints (night guards): Devices worn over the teeth during sleep to reduce clenching forces and reposition the jaw. These are among the most commonly used interventions for bruxism-related TMD.
Physical therapy: Exercises and manual techniques targeting jaw muscles and cervical posture are part of standard care for TMD in many clinical settings.
Behavioral interventions: Awareness-based techniques to reduce daytime clenching, jaw muscle tension, and postural habits that load the TMJ.
Dietary modification: Temporarily reducing chewing load (soft foods) during acute TMD flares reduces mechanical stress.
For the tinnitus component, the same evidence-based tools used for other tinnitus types, including sound therapy and cognitive behavioral approaches, are applicable and can reduce distress while jaw treatment proceeds.
The evidence base for direct causal treatment of TMJ-related tinnitus remains limited in scope. Most guidelines recommend a conservative, reversible approach before considering more invasive interventions on the jaw joint. Multidisciplinary evaluation involving both a TMD specialist and an audiologist provides the most complete assessment for people in whom the jaw is suspected as a significant contributor.
The overlap with bruxism
Bruxism, the habit of clenching or grinding the teeth, often coexists with both TMD and tinnitus. Grinding places repetitive compressive load on the TMJ and surrounding muscles during sleep, when the person cannot consciously moderate the force. Over time this contributes to TMJ disc displacement and muscle hypertonicity.
People with bruxism-related TMD may notice that their tinnitus is at its worst in the morning, immediately after sleep when the effects of overnight grinding are most acute. This timing pattern, combined with jaw soreness, headache upon waking, or a partner noticing grinding sounds, points toward bruxism as a contributing factor that warrants discussion with a dentist experienced in sleep-related jaw conditions.
When to seek evaluation
A combined evaluation involving an audiologist for the tinnitus component and a clinician experienced in TMD for the jaw component is the appropriate starting point when TMJ-related tinnitus is suspected. The audiologist can establish hearing baselines, screen for cochlear contributors, and provide tinnitus management tools. The TMD clinician can assess joint mechanics, disc position, and muscle function using clinical examination and, where needed, imaging of the joint.
Neither specialist should be bypassed in favor of treating only one component of what is often a multifactorial presentation.
If symptoms persist or change, see an audiologist or physician.
Frequently asked questions
- If my tinnitus changes when I clench my jaw, does that mean it's definitely TMJ-related?
- Modulation of tinnitus by jaw clenching is a marker of somatosensory involvement, but it does not by itself confirm a TMJ diagnosis. Many people with noise-induced tinnitus also show some degree of somatic modulation. A full evaluation by a clinician familiar with both audiology and temporomandibular disorders is needed to determine whether TMJ is the primary driver.
- Will treating my TMJ disorder cure my tinnitus?
- Evidence suggests that managing the TMJ component can reduce tinnitus severity in people where the jaw is a significant contributor. However, complete resolution is not guaranteed, particularly if other cochlear or central factors are also involved. Evidence in this area is limited and outcomes vary between individuals.
- Can a dentist or oral surgeon help with TMJ-related tinnitus?
- Dentists and oral surgeons with training in temporomandibular disorders are appropriate specialists to evaluate TMJ function. Management of the jaw component may involve occlusal splints, physical therapy for the jaw musculature, or postural correction. Coordination with an audiologist for the tinnitus component is often part of a multidisciplinary approach.
EarLabs Notes
One short note a week. Tinnitus and hearing health.
New tools, plain-language summaries of recent research, no spam. Unsubscribe in one click.
No tracking pixels, no behavioral retargeting. Read our privacy notes.
Primary sources
- Tinnitus - NIDCD — National Institute on Deafness and Other Communication Disorders
- Temporomandibular Joint Disorders - NIH — National Institute of Dental and Craniofacial Research, NIH
- Tinnitus - Mayo Clinic — Mayo Clinic
- Clinical Practice Guideline: Tinnitus - AAO-HNS — American Academy of Otolaryngology, Head and Neck Surgery