frequencies
What pitch is your tinnitus, and what your answer reveals about its source
Tinnitus pitch usually mirrors the frequency of your hearing loss. How to estimate your tinnitus pitch with a free online tone generator and why it correlates with cochlear damage location.
Published May 21, 2026 · By the EarLabs editorial desk
Most people can describe their tinnitus in broad terms: it sounds like ringing, hissing, buzzing, or a high-pitched whine. Fewer people know the approximate frequency of their tinnitus, but that number is more informative than it might seem.
Tinnitus pitch is not random. It correlates with the location of cochlear damage and with the frequency region of hearing loss. Knowing roughly where your tinnitus sits on the frequency spectrum can help explain why it sounds the way it does and, in some treatment approaches, helps clinicians tailor sound-based interventions.
How the cochlea encodes frequency
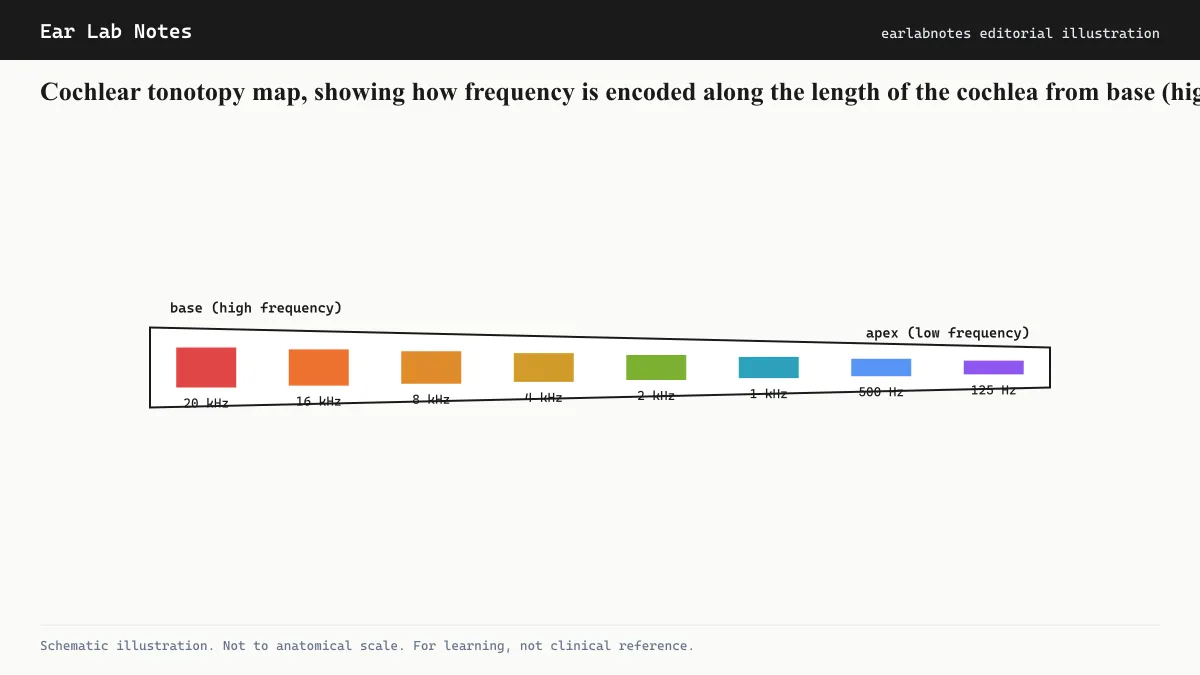
The cochlea is a coiled structure in the inner ear, roughly the size of a pea. One of its most important properties is that it encodes frequency spatially, a quality called tonotopy.
High frequencies are detected at the base of the cochlea, the wide end near the oval window. Low frequencies are detected at the apex, the center of the coil. Every frequency in between maps to a specific location along the basilar membrane that runs the length of the cochlea.
This spatial organization extends throughout the auditory system, into the auditory nerve, brainstem nuclei, and auditory cortex. Each level of the auditory pathway maintains its own tonotopic map.
When hair cells at a specific cochlear location are damaged, the auditory neurons that served that frequency region lose their normal input. According to the central-gain model, these neurons may then increase their spontaneous firing rate to compensate. The brain interprets that elevated firing as a sound from that frequency region, which becomes the tinnitus.
Where tinnitus pitch tends to sit
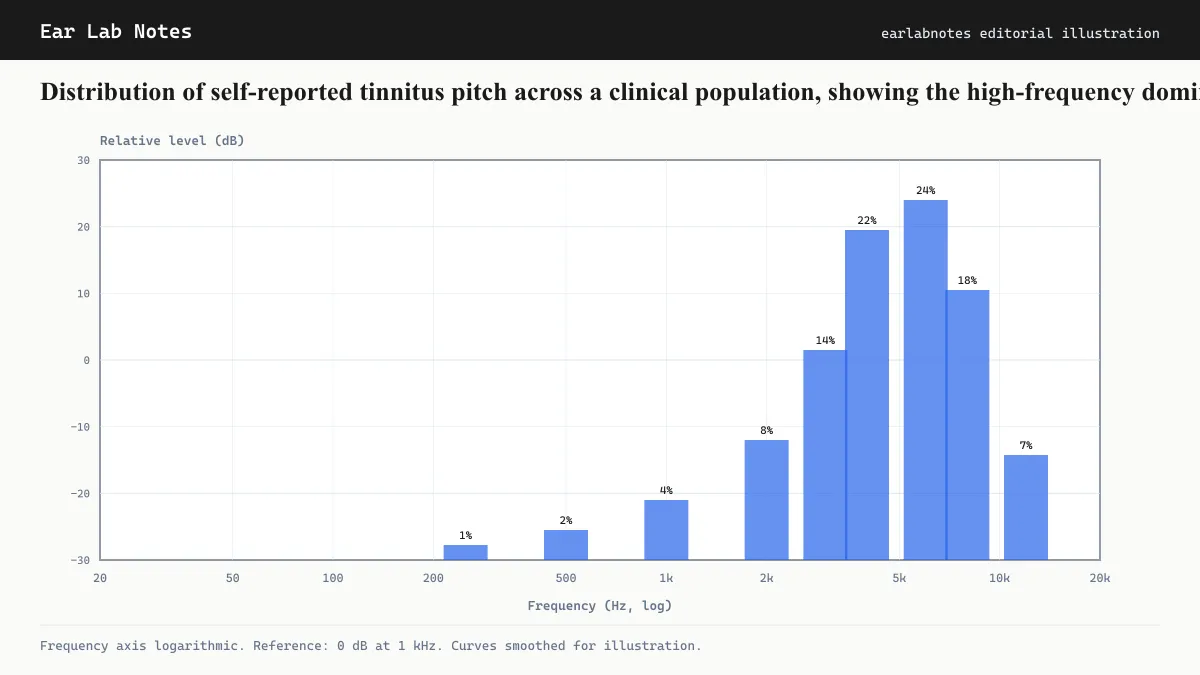
Across clinical populations, tinnitus pitch is not distributed evenly across the audible range. It clusters heavily in the high frequencies.
The most commonly reported pitches fall between 3,000 Hz (3 kHz) and 8,000 Hz (8 kHz). This matches the frequency region that is most vulnerable to damage from both noise exposure and age-related hearing loss (presbycusis).
The reason this region is vulnerable has to do with the mechanics of the cochlea and the intensity of sounds in everyday environments. The 4 kHz region in particular is where noise-induced damage typically appears first, a pattern that shows up as the characteristic “noise notch” on audiograms and corresponds to the most common tinnitus pitch reported in clinic.
Pitch matching: how audiologists measure it
Formal tinnitus pitch matching is a psychoacoustic procedure. An audiologist plays test tones of known frequencies and asks the patient to indicate which sounds most closely resemble their tinnitus. The procedure usually narrows down through several rounds from broad frequency ranges to a narrower estimate.
Pitch matching can also be performed by patients at home using freely available tone-generator websites or apps. Many people find this gives a useful rough estimate. But informal home pitch matching has limitations:
- Headphone frequency response varies widely and may distort the result
- The tinnitus may not perfectly resemble a pure tone, making comparison difficult
- Psychoacoustic phenomena like octave confusion (where tinnitus at one frequency is misjudged by one octave) are common
The BTA notes that tinnitus rarely sounds like a pure sine wave. It may be narrowband noise, or have tonal qualities, making exact pitch matching inherently imprecise.
The edge effect: why tinnitus sits near the edge of hearing loss
A consistent finding in tinnitus research is that tinnitus pitch tends to sit at or just above the edge of the region of hearing loss. This is called the edge effect.
The explanation fits neatly with the central-gain model. Hair cells at the exact boundary of damage are the neurons most affected by the contrast between normal input on one side and absent input on the other. This boundary region may show the highest levels of compensatory spontaneous activity, producing the strongest phantom signal.
This means that pitch matching may serve as an indirect indicator of where hearing loss begins, even before that loss shows clearly on a standard audiogram. Research groups studying cochlear synaptopathy (hidden hearing loss) have used this observation to investigate early cochlear damage.
What your pitch estimate tells you
If your tinnitus sits at around 4 kHz to 6 kHz (a sharp, high-pitched whistle or ring), this pattern is consistent with noise-induced hearing loss. The NIDCD and NIOSH both document this as the most common audiometric and tinnitus-frequency pattern following occupational or recreational noise exposure.
If your tinnitus is higher still, above 8 kHz, it may correspond to extended high-frequency hearing loss that a standard audiogram (which typically tests up to 8 kHz) does not capture. Extended high-frequency audiometry, offered by some specialist audiology clinics, can assess this range.
If your tinnitus is low-pitched, below about 1 kHz, this pattern is less common and more often associated with specific conditions. Meniere’s disease characteristically produces a low-pitched roaring or rumbling tinnitus that often fluctuates with fluid pressure changes in the inner ear. Eustachian tube dysfunction can also produce a low-frequency sensation.
Limitations of pitch matching as a diagnostic tool
Pitch matching, while informative, has recognized limitations. The correlation between tinnitus pitch and audiogram patterns is strong at a population level but imperfect at the individual level. Some people report tinnitus pitches that do not correspond to their region of greatest hearing loss.
Additionally, tinnitus is not always a single pitch. Compound tinnitus, where multiple distinct pitches or noise bands are perceived simultaneously, is common. Matching one component may miss others.
For these reasons, tinnitus pitch matching is one data point in a broader audiological evaluation, not a standalone diagnostic test. Audiologists typically combine it with a standard audiogram, loudness matching, and clinical history.
If symptoms persist or change, see an audiologist or physician.
Frequently asked questions
- Can I accurately identify my tinnitus pitch at home?
- Online pitch-matching tools and tone generators can give a rough estimate, but they are not clinically precise. Headphone quality, room acoustics, and the psychoacoustic difficulty of matching a narrow-band internal sound to a pure tone all introduce variability. A formal pitch match performed by an audiologist using calibrated equipment is more accurate.
- Does the pitch of tinnitus ever change?
- Yes. Tinnitus pitch can fluctuate, sometimes from hour to hour, particularly in conditions like Meniere's disease. Noise exposure, stress, and fatigue can also shift the perceived pitch. For this reason, clinical pitch-matching results are considered estimates rather than fixed measurements.
- What does a very high pitched tinnitus (above 8 kHz) suggest?
- Very high-frequency tinnitus often corresponds to hearing loss in the extended high-frequency range, which standard audiograms (tested to 8 kHz) may not fully capture. It can be associated with early noise damage or age-related changes in the basal cochlea. An audiologist can assess extended high-frequency thresholds if indicated.
- Is low-pitched tinnitus less common?
- Yes. Most tinnitus clinical populations report high-frequency pitches. Low-pitched tinnitus (below about 1 kHz) is less common in the general tinnitus population and is more associated with specific conditions like Meniere's disease, eustachian tube dysfunction, and some vascular causes.
- Does matching my tinnitus pitch help with treatment?
- Pitch matching is used in tinnitus retraining therapy, notched music therapy, and some masking approaches, where knowing the approximate frequency helps tailor the sound therapy. However, its clinical use varies by treatment protocol. Consult an audiologist about whether pitch matching is relevant to your management plan.
EarLabs Notes
One short note a week. Tinnitus and hearing health.
New tools, plain-language summaries of recent research, no spam. Unsubscribe in one click.
No tracking pixels, no behavioral retargeting. Read our privacy notes.
Primary sources
- Tinnitus — NIH/NIDCD
- Clinical Practice Guideline: Tinnitus — American Academy of Otolaryngology - Head and Neck Surgery (AAO-HNS)
- Hearing, Ear Infections, and Deafness — NIH/NIDCD
- About Tinnitus — British Tinnitus Association (BTA)