science
Why hearing loss causes ringing: the central-gain hypothesis
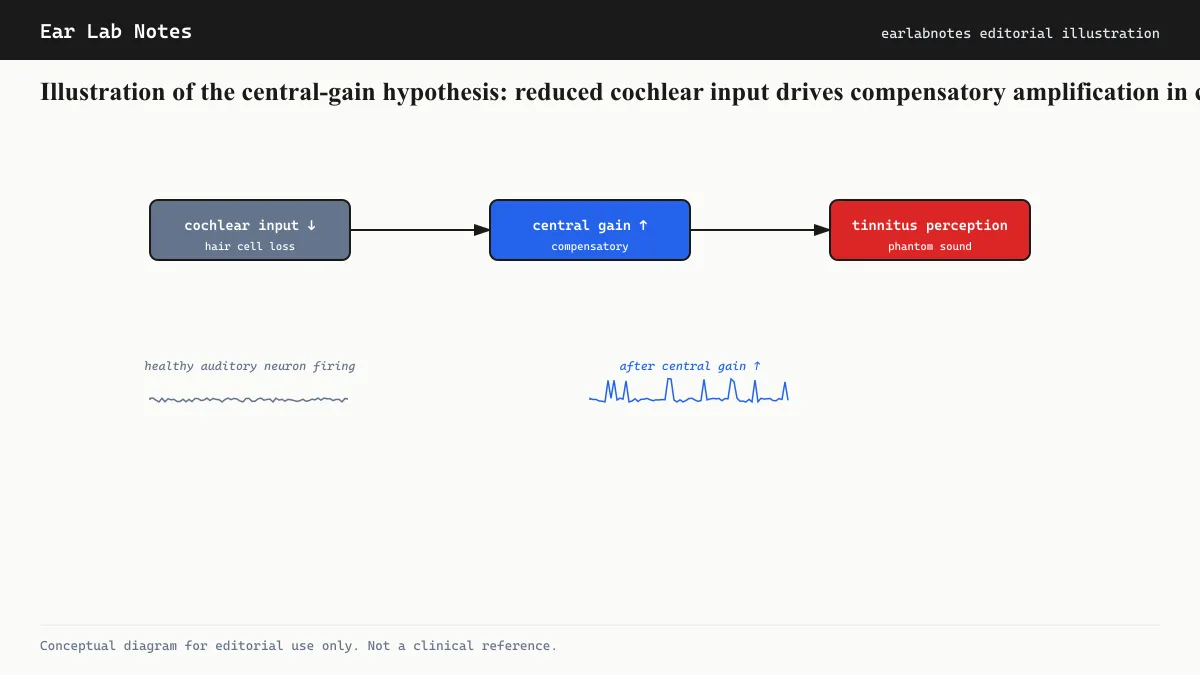
When the cochlea sends less signal, the brain's auditory pathway turns up its gain. That gain amplifies internal noise into perceptible ringing. The current dominant model explained.
Published May 21, 2026 · By the EarLabs editorial desk
The puzzle at the center of tinnitus research
Most people with tinnitus also have some degree of hearing loss. Most people with hearing loss do not have tinnitus. The relationship is strong enough to be epidemiologically clear but too inconsistent to be a simple causal rule. Understanding why hearing loss so often produces tinnitus requires going beyond the ear itself, into the auditory brain.
The central-gain hypothesis is the current dominant model for this relationship. It draws on well-established principles of neural adaptation to explain how the brain’s compensatory response to reduced cochlear input can produce phantom sound.
Gain as a biological concept
In electronics, gain is the ratio of output to input. Amplifiers with high gain boost a weak signal; those with low gain let strong signals pass without amplification. Biological neural systems use analogous mechanisms.
When sensory input decreases, the nervous system often compensates by increasing its sensitivity to whatever input remains. This is homeostatic plasticity, the brain’s tendency to regulate its own excitability to maintain useful function. It occurs in the visual system, the somatosensory system, and the auditory system.
In the auditory pathway, this compensation can operate at multiple levels: the dorsal cochlear nucleus, the inferior colliculus, the medial geniculate body of the thalamus, and the auditory cortex. Each of these stations can, under certain conditions, increase its responsiveness when the input arriving from lower stations is reduced.
How cochlear hair cell loss creates the conditions for tinnitus
When cochlear hair cells in a particular frequency region are damaged or destroyed, the auditory nerve fibers serving that region lose their normal stimulation. The spontaneous firing rate of those nerve fibers typically decreases, and their input to the central auditory stations is reduced.
The central stations respond. Research in animal models has documented increased spontaneous firing rates in the cochlear nucleus, inferior colliculus, and auditory cortex after cochlear hair cell loss. The neurons at these levels become more easily excited even in the absence of sound, generating neural activity that the brain has no way to distinguish from activity driven by real sounds.
This increased spontaneous activity in auditory neurons corresponds, in the subjective experience of a person, to a sound that is not there. It is perceived as ringing, hissing, buzzing, or other sounds at the frequency that the damaged cochlear region previously processed.
NIDCD has described this mechanism as one of the leading explanations for why tinnitus so commonly accompanies sensorineural hearing loss, and why the pitch of tinnitus so often aligns with the frequency region of greatest hearing loss.
The inhibition balance shift
A more specific version of the gain hypothesis focuses on inhibition. The central auditory pathway uses a combination of excitatory and inhibitory signaling to process sounds. Inhibitory interneurons, which release the neurotransmitter GABA among others, suppress neural activity to reduce background noise and sharpen signal processing.
When peripheral input is reduced, inhibitory signaling in the auditory pathway may decrease disproportionately. This shifts the balance toward excitation. Neurons that would normally be held quiet by inhibitory inputs become more active. The result is increased spontaneous activity that may be out of proportion to what a straightforward amplification of input would predict.
This inhibitory-loss mechanism helps explain findings from animal research in which tinnitus behaviors correlate with reductions in GABA-ergic inhibition in auditory brainstem nuclei. It also suggests potential pharmacological targets, though no treatment based on restoring inhibitory tone has yet achieved clinical validation for tinnitus.
Why frequency-specific damage produces frequency-specific tinnitus
The cochlea’s tonotopic organization, its mapping of frequency to physical location, is preserved through the entire auditory pathway up to the cortex. Each stage of the auditory system maintains the frequency-to-location map. This means that damage at a particular cochlear location disrupts input to a corresponding location in the central auditory map.
The increased spontaneous activity generated in response to that reduced input is therefore not random. It is concentrated in neurons tuned to the frequency range of the damaged cochlear region. The brain registers it as sound at that frequency. This predicts, and observations confirm, that people’s tinnitus pitch tends to cluster near the upper edge of their audiometric hearing loss notch.
The upper edge of the notch, rather than the center, is the most common tinnitus pitch because the neurons at the frequency boundary between damaged and undamaged cochlear regions may be partially deafferented (losing some inputs) while still receiving some input, creating the conditions for hyperactivity rather than simply silence.
Evidence from clinical observations
Several clinical observations support the central-gain model:
Hearing aids and tinnitus. Many people report that fitting appropriately programmed hearing aids, which restore auditory input across the impaired frequency range, reduces their tinnitus perception. This is consistent with the prediction that providing more real input reduces the drive for central gain amplification.
Cochlear implants and tinnitus. A majority of cochlear implant recipients report reduced or eliminated tinnitus in the implanted ear during device use, even though cochlear implant electrodes do not restore the cochlea’s native hair cells. Providing electrical stimulation of the auditory nerve reduces tinnitus, again consistent with the central-gain model.
Single-sided deafness. People who lose all hearing in one ear often develop tinnitus in that ear, or in both ears. The total loss of cochlear input from one side provides the extreme case: maximum central gain, no peripheral input, and a high rate of tinnitus.
Night-time amplification. When background sound levels fall at night, the contrast between phantom sound and silence increases, and tinnitus seems louder. This is not gain in the central-gain sense, but it illustrates how reduced environmental input changes the salience of any internal signal.
The model’s limits
The central-gain hypothesis explains a great deal, but not everything. Key open questions include:
Why do some people with similar audiometric profiles develop severe, distressing tinnitus while others do not, or have only mild tinnitus? The gain model predicts greater amplification with greater hearing loss, but the relationship is imperfect.
Why does tinnitus sometimes persist after cochlear nerve section? If the cochlea is the source of reduced input driving central gain, removing the nerve entirely should eliminate the drive. That it sometimes does not suggests that once established, the central abnormality can become self-sustaining.
NIDCD-funded research programs continue to investigate these questions, with the aim of identifying more precise targets for intervention within the central auditory pathway.
If symptoms persist or change, see an audiologist or physician.
Frequently asked questions
- Does everyone with hearing loss get tinnitus?
- No. Hearing loss significantly increases the risk of tinnitus, but many people with measurable hearing loss on an audiogram never develop tinnitus. Why some people do and others do not is an active research question. Factors including the degree of hearing loss, the frequency range affected, and individual differences in central auditory processing appear to play a role.
- Can you have tinnitus without hearing loss?
- Yes. A standard audiogram may appear normal in some people with tinnitus, particularly early in the course of noise-induced damage. Research has established that cochlear synaptopathy (damage to the synapses between hair cells and auditory nerve fibers) can be present before audiometric thresholds shift. Hidden hearing loss of this kind may contribute to tinnitus even when standard tests look normal.
- If treating hearing loss makes tinnitus better, what does that mean?
- It is consistent with the central-gain hypothesis. If tinnitus results partly from the brain amplifying its response to reduced input, providing more real input through hearing aids or cochlear implants would reduce the drive to amplify. Many people report reduced tinnitus after fitting hearing aids that are appropriate to their hearing loss, though individual results vary.
- Is the central-gain hypothesis proven?
- It is the dominant model, supported by multiple lines of evidence including animal physiology, human neuroimaging, and clinical observations. It is not the only explanation for tinnitus, and it almost certainly works together with other mechanisms including cortical map reorganization and limbic system involvement. No single theory explains all cases.
- What is the endocochlear potential and how does it relate to tinnitus?
- The endocochlear potential is a standing voltage of roughly +80 millivolts in the endolymph relative to perilymph, maintained by the stria vascularis. It provides the driving force for potassium influx into hair cells. When cochlear blood supply is compromised (by aging, noise, or ototoxic drugs), the endocochlear potential decreases, reducing hair cell signaling and contributing to the conditions that produce tinnitus through central gain.
EarLabs Notes
One short note a week. Tinnitus and hearing health.
New tools, plain-language summaries of recent research, no spam. Unsubscribe in one click.
No tracking pixels, no behavioral retargeting. Read our privacy notes.
Primary sources
- Tinnitus: Overview and Management — NIH/NIDCD
- Noise-Induced Hearing Loss — NIH/NIDCD
- Tinnitus: Symptoms and Causes — Mayo Clinic
- Clinical Practice Guideline: Tinnitus — AAO-HNS